Background: Diagnosis is complex, dynamic, and high risk for harmful errors in the inpatient setting. It is critical to understand daily workflows and the adaptations that create a safe and resilient diagnostic process, though this is challenging using traditional research methods alone. The aim of this ethnographic study is to identify and analyze personal, team, and system factors that support a successful diagnostic process.
Methods: We conducted observations during clinical shifts using a standardized data collection form followed by semi-structured interviews and focus groups with clinicians post-shift. Each observation session took place during the day on teaching and non-teaching general medicine services, covering different activities including pre-rounding, rounding, and afternoon clinical work. A preliminary thematic analysis of interview data and structured observation field notes was conducted to inform the design of potential future diagnostic process interventions.
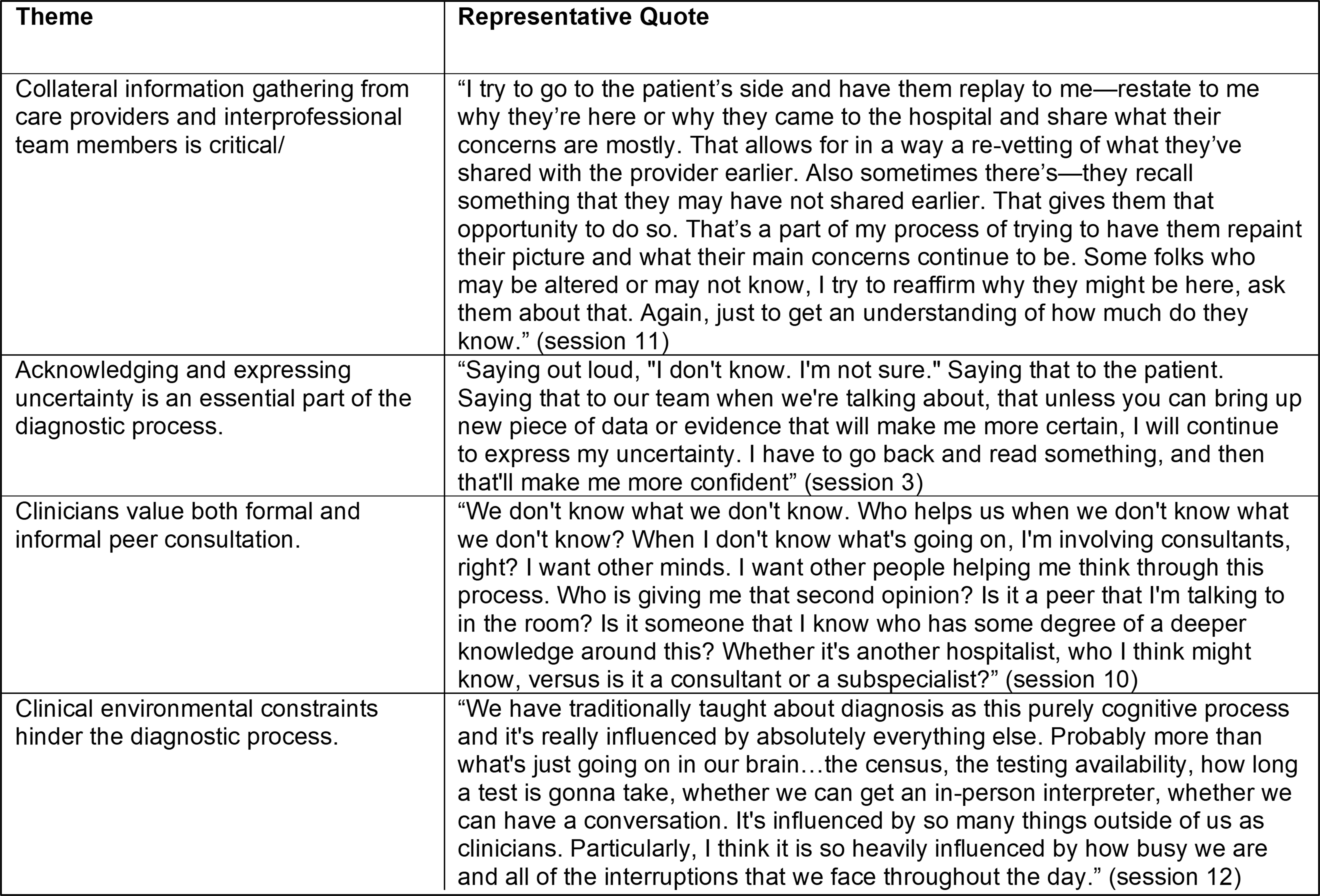
Results: We observed twelve teams at six academic hospitals while rounding on 96 patients for 120 hours. We conducted twelve interviews with 20 providers (two advanced practice providers, six medical students or residents and twelve attending physicians). Using field notes and a preliminary thematic analysis of interview transcripts, four preliminary themes were identified: 1) Collateral information gathering from care providers and interprofessional team members is critical, 2) Acknowledging and expressing uncertainty is an essential part of the diagnostic process, 3) Clinicians value both formal and informal peer consultation and 4) Clinical environmental constraints hinder the diagnostic process.
Conclusions: Based on preliminary analysis, interventions to support accurate diagnosis and adaptation may consider mechanisms to formalize collaboration with peer clinicians, interprofessional team members, and patients. Developing a hospitalist workforce capable of navigating diagnostic uncertainty and removing systems barriers may also contribute to better diagnosis. A formal rapid qualitative analysis including templated summaries, matrix analysis, and triangulation of interviews with observation field notes is underway to elucidate cross-cutting themes and subthemes.