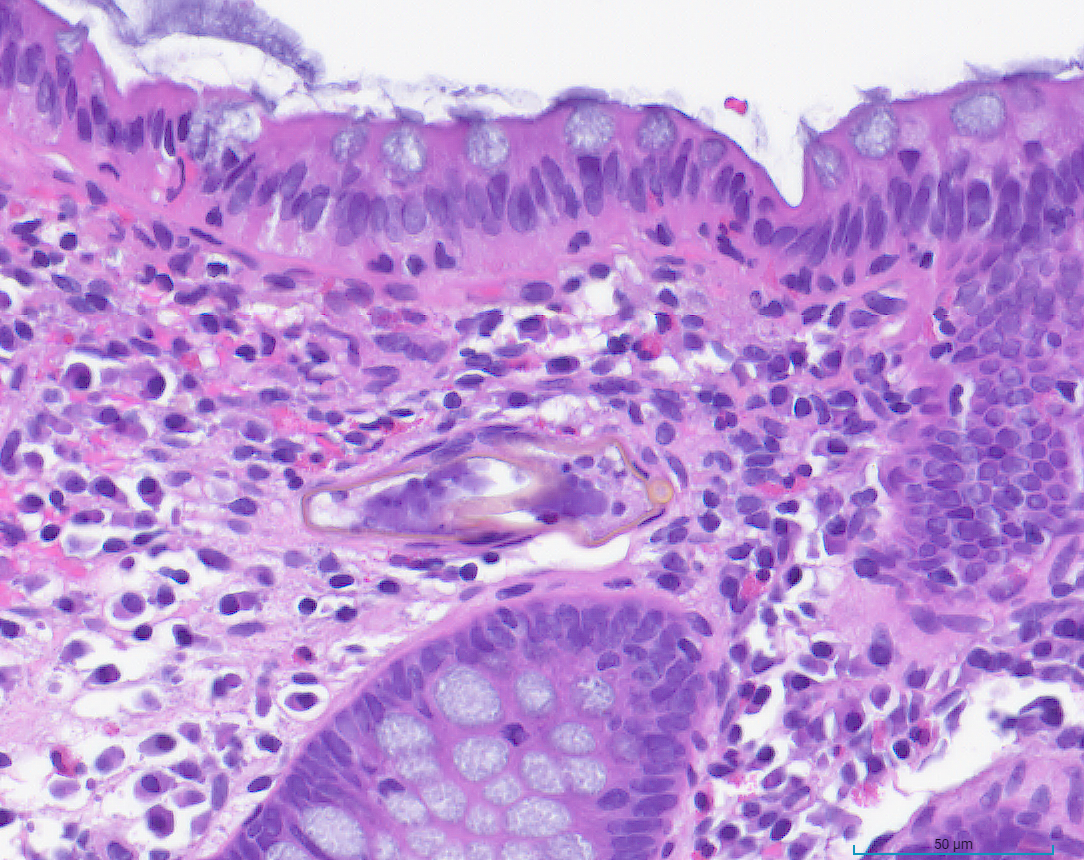
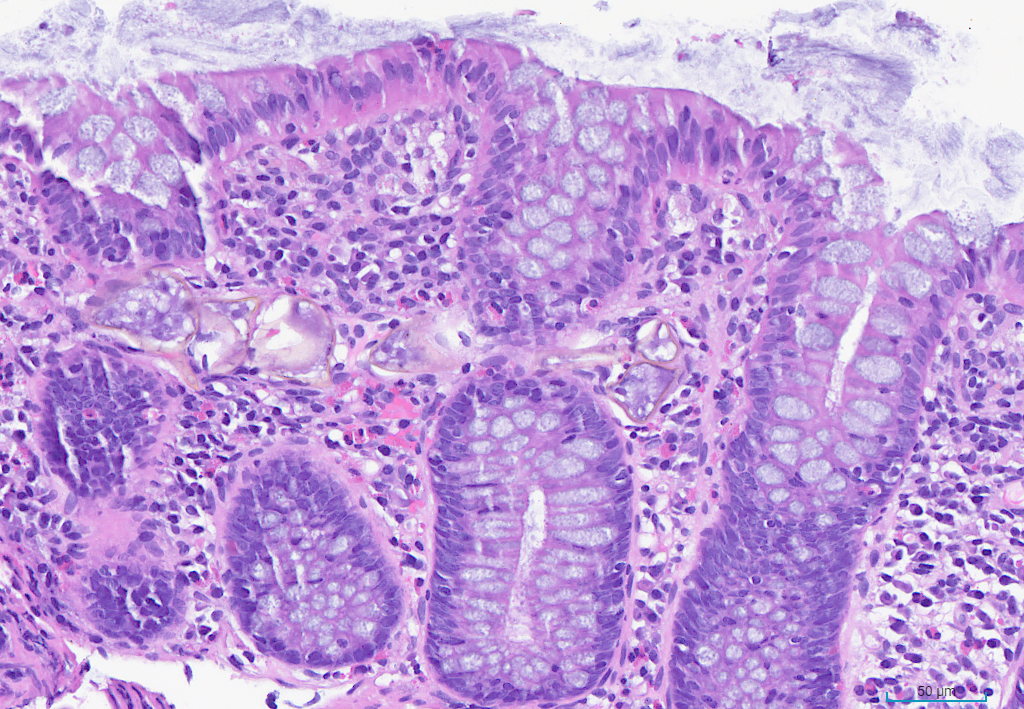
Case Presentation: An 18-year-old male with a history of Hepatitis B presented to the ED with 1 month of low-grade fevers, bilateral lower extremity arthralgias (knees, hips, lumbar spine), and 5 days of rectal bleeding. Originally from Guinea, he recently emigrated from Nicaragua. He reported 9/10 joint pain, which started in the left foot and ascending to the hips and lumbar spine, accompanied by intermittent fevers. He denied trauma, nausea, vomiting, diarrhea, or family history of colorectal cancer but noted dark, red-streaked stool for 5 days. Physical exam revealed bilateral knee and hip tenderness with limited ROM, and redness on the soles, abdominal exam benign. Labs revealed iron-deficiency anemia (Hgb 8.1, HCT 29.1, MCV 60.3, iron 16, transferrin 4.36), mild inflammatory markers (ESR 28, CRP 6.9), and negative autoimmune markers (ANA, ANCA, CCP, Ro/La, DS-DNA). Imaging showed erosive sacroiliac (SI) joint changes consistent with seronegative spondyloarthropathy. Active hematochezia prompted colonoscopy, intra-op findings initially suggested pancolitis ulcerative colitis (UC), and IV methylprednisolone was started. However, GI PCR later identified E. histolytica, prompting metronidazole initiation and steroid cessation. Biopsies finally confirmed parasitic ova indicating schistosomiasis instead of UC. He was treated with praziquantel. On discharge, paromomycin was recommended for intraluminal coverage, and he was set up for follow-ups.
Discussion: Schistosomiasis is a parasitic infection caused by waterborne trematodes, which consists of three main species that infect humans: S. mansoni, S. haematobium, and S. japonicum, all prevalent in different regions of the world, but most common in sub-Saharan Africa, South America, East Asia, and the Middle East. Acute infection with schistosomiasis manifests nonspecifically—commonly as intermittent fever, generalized rash, intermittent cough, and gastrointestinal complaints. Chronic infection, however, ranges from asymptomatic to fulminant disease and can manifest as liver disease, pulmonary fibrosis, bladder calcification, gastrointestinal disease, neuroschistosomiasis, etc. Although the aforementioned symptoms are well-documented, arthropathy is rarely reported. The first detailed findings of schistosomiasis-related arthropathy were described by El-Bassiouni. To date, reactive arthritis following parasitic infections has been infrequently studied, with schistosomiasis being among the least documented.
Conclusions: In patients with migrating joint pain and new-onset hematochezia, inflammatory bowel disease (IBD) has been the prevailing diagnosis among teams. For this patient, bilateral SI joints with patterns of seronegative spondyloarthropathy on imaging, as well as colonoscopy findings consistent with UC, increased the pretest probability for IBD. However, recognizing infectious causes in immigrant patients proved vital to an accurate diagnosis, particularly in this case. Shortly after the colonoscopy, GI PCR revealed Entamoeba histolytica, which prevented the continuation of empiric steroid treatment and cast doubt on a preliminary UC diagnosis. Ultimately, pathology revealed Schistosoma ova within the lamina propria. Additionally, HLA-B27 positivity is often associated with a higher risk of reactive polyarthritis. These critical findings, alongside the patient’s migrating polyarthropathy, provided a strong argument for reactive arthritis from schistosomiasis as the ultimate diagnosis.