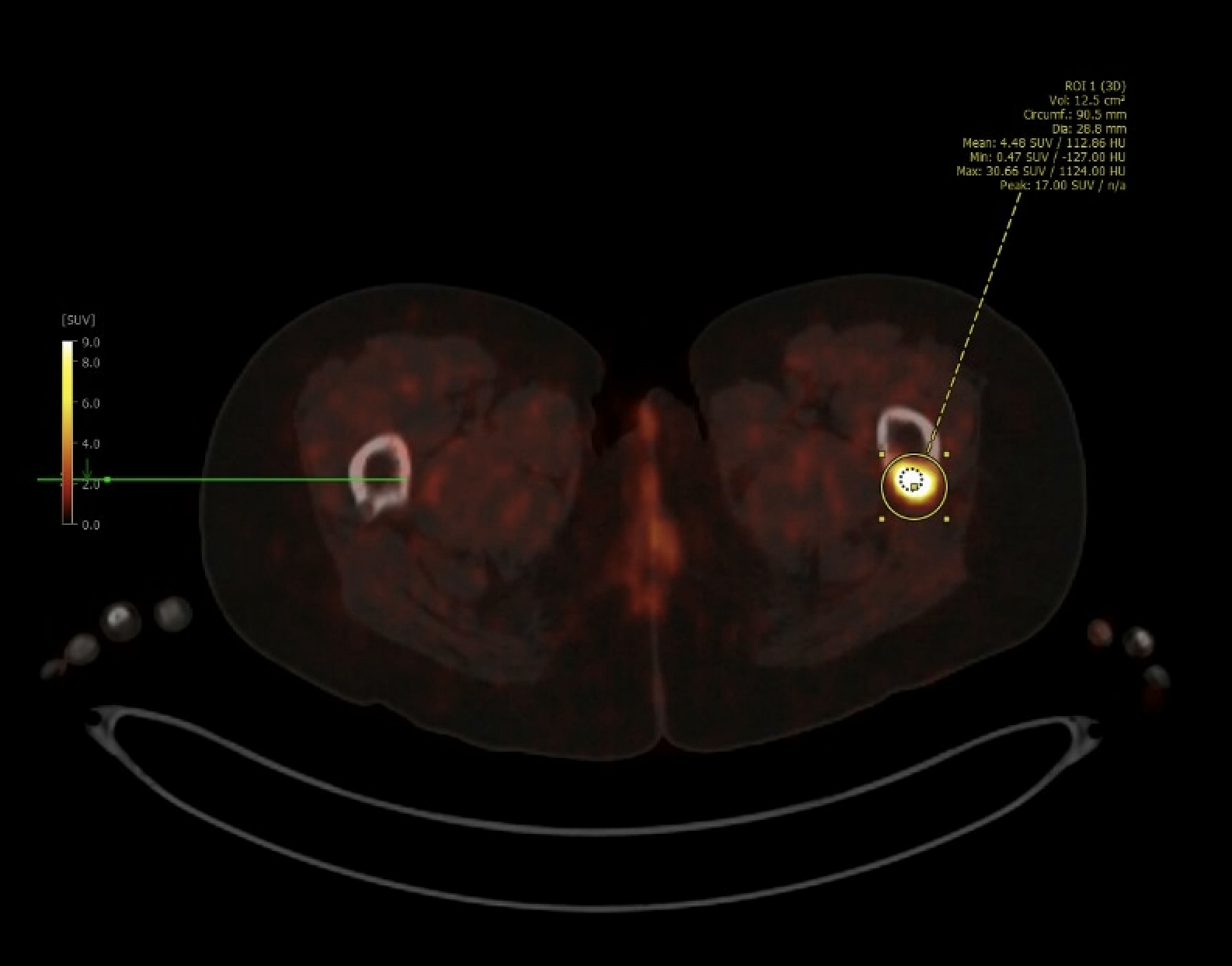
Case Presentation: A 38-year-old woman with a history of recent pelvic fractures presented for admission per her primary care physician due to progressive hip pain and difficulty ambulating, with the hope of expediting a diagnosis of the underlying etiology. Patient had had multiple recent presentations with similar complaints. Imaging studies prior to admission revealed bilateral iliac fractures, osteonecrosis of both femoral heads, and osteolytic lesions of the pelvis. She had been evaluated by Oncology but malignancy workup including CT chest/abdomen/pelvis, SPEP/UPEP, and peripheral flow cytometry, had been unrevealing. Further laboratory studies revealed an elevated alkaline phosphatase, markedly low phosphorus, and elevated fibroblast growth factor 23 (FGF23), raising suspicion for tumor-induced osteomalacia, though without clear evidence of a tumor up to that point. While admitted, we attempted to identify/localize a tumor with a gallium-68 DOTATATE PET scan, but were not permitted to perform this inpatient. Instead, we adjusted patient’s pain regimen to achieve adequate control, supplemented her persistently low phosphorus level, had her work with physical and occupational therapy, and expedited outpatient imaging. She discharged home and was able to obtain the PET scan soon after discharge, which revealed a tracer-avid focus in the left proximal femur. She subsequently underwent excision and pathology revealed a mesenchymal tumor. Afterwards, she experienced normalization of her phosphorus and FGF23 levels, and slow improvement in her pain and mobility.
Discussion: Tumor-induced osteomalacia is a rare entity where mesenchymal tumors produce FGF23, causing decreased reabsorption of phosphate by the kidney, resulting in osteomalacia, bone pain, muscle weakness, and fractures [1]. Identifying the tumor can be difficult due to their typical slow growth, small size, and often obscure anatomical locations. Resection of the tumor is curative with normalization of biochemical changes and improvement in bone health and functional status [2]. Nuclear medicine imaging is typically needed to identify these tumors [3], such as the gallium-68 DOTATATE study performed for this patient. In this case, this study was attempted inpatient, but due to cost and limited nuclear material, we were not allowed to perform this inpatient. Rather, we stabilized the patient, controlled her symptoms, assessed her functional capacity and safety, and expedited further outpatient workup that ultimately resulted in identification of the tumor and resolution of her issues.
Conclusions: The diagnosis of tumor-induced malacia often requires an extensive workup to identify the tumor. A common misconception among physicians and patients is that admission to the hospital will expedite complex diagnostic workups such as this. In this case, due to the cost of and limited availability of nuclear resources, inpatient admission was actually a barrier to this patient getting the testing she needed. While admission was appropriate to control patient’s symptoms and ensure she was safe from a functional standpoint, the definitive diagnosis and resolution to her issues were accomplished outside of the hospital. A thorough understanding of what can and cannot be accomplished through hospitalization is important for hospitalists.