
Background: Gastrointestinal (GI) malignancies are a leading cause of cancer mortality accounting for ~28% of cancer deaths in the U.S. [1]. Perforation, peritonitis, and septic shock are severe complications often presenting later in the disease course and associated with surgery, prolonged hospitalization, and mortality [2]. Social determinants of health (SDOH) including race, socioeconomic status, and insurance are linked to advanced stage diagnosis, higher rates of emergency presentations, and worse survival [3]. Limited data details how SDOH influence the risk of perforation, peritonitis, and sepsis among patients with established GI cancers or how they affect in-hospital outcomes. We evaluated SDOH-associated differences in these complications and examined their impact on inpatient mortality and resource utilization.
Methods: Using the National Inpatient Sample (2018–2021), we conducted a retrospective study and identified adults ≥ 18 years with GI malignancies via ICD-10 codes and categorized them as esophageal, gastric, small bowel, colorectal, hepatobiliary, pancreatic, or Other GI cancers. Primary outcomes were inpatient perforation/peritonitis and sepsis/septic shock. Predictors included age, sex, race, insurance, income, and cancer site. Secondary outcomes were length of stay (LOS), hospital charges, and discharge disposition. Survey-weighted regression generated adjusted odds ratios (aORs) with 95% CIs using White race, Medicare, lowest income quartile, and esophageal cancer as references.
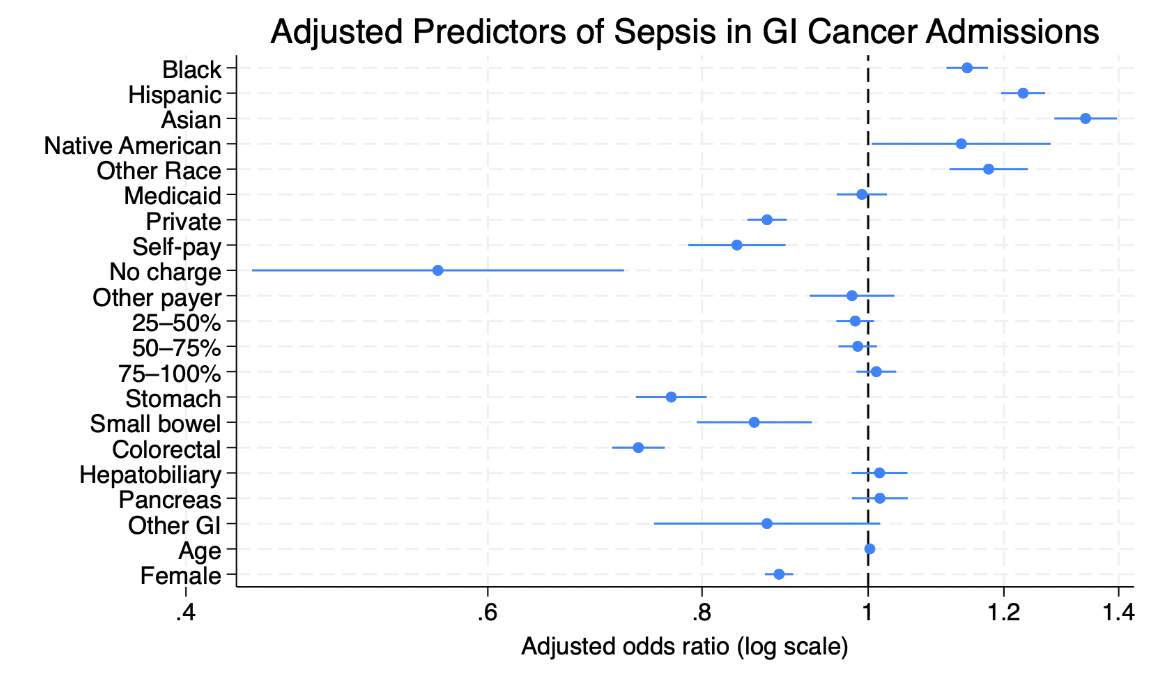
Results: Black and Hispanic patients had lower odds of perforation/peritonitis (15% and 13%), while Medicaid and self-pay had higher odds (24% and 18%). All cancer sites except hepatobiliary demonstrated increased risk, highest in small-bowel cancers (346%). For sepsis, Black, Hispanic, Asian, and Other groups had higher odds (14–34%), while private insurance and no-charge encounters had lower odds (12% and 59%). Septic shock results paralleled sepsis.Longer LOS was associated with Black, Hispanic, Asian, and Other groups (all p< 0.05), Medicaid and self-pay (p≤0.001), lower income (p< 0.001), female sex (p< 0.001), older age (p< 0.001), and stomach, small-bowel, hepatobiliary, pancreatic, and other GI cancers (p≤0.01). Shorter LOS occurred with private insurance, higher-income quartiles, and colorectal cancer (all p< 0.001).Hospital charges were higher for Black, Hispanic, Asian, and Other groups (p< 0.05), lower across all payer groups (all p≤0.001), increased with income (p< 0.001), and were higher in small-bowel, colorectal, stomach, and other GI cancers, but lower in hepatobiliary and pancreatic cancers (all p≤0.01). Discharge to a facility was more likely among Black patients and those with higher income (p< 0.001) and less likely among Hispanic, Asian, and Other groups (p< 0.001). All payer groups had lower odds (p< 0.001), and all malignancies had lower odds of facility care (p<.002).
Conclusions: SDOH influence the outcomes of acute complications in GI malignancies. Insurance, income, and race were associated with differing risks of perforation, peritonitis, sepsis/septic shock, and variation in resource use and post-acute care requirements. Furthermore, structural factors contribute to life-threatening complications and hospitalization outcomes. Targeted interventions that reduce diagnostic delays, expand outpatient oncology access, and address financial/geographic barriers are essential to reducing inequities and improving inpatient outcomes.
.png)