Background: Beginning in 2023, our urban community teaching hospital identified improving efficiency as a key strategic priority. One specific goal was to improve our average inpatient length of stay (LOS) which was reported as higher than both local and national peer institutions, based on observed-to-expected LOS (O/E) and case mix index (CMI) adjusted. Executive leadership convened multidisciplinary focus groups which led to the identification of standardization and optimization of interdisciplinary rounds (IDRs) as a key strategy to reduce LOS and improve care progression.
Purpose: To implement a standardized IDR model on all inpatient medicine units to reduce LOS and improve care progression.
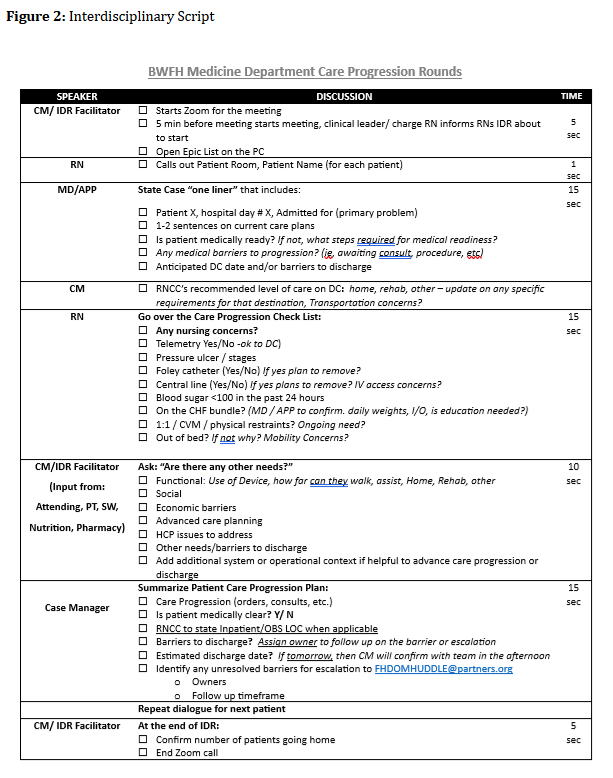
Description: Our hospital has conducted unit-based IDRs for more than 10 years. However, IDR practices were not standardized across units, and content and participation varied across locations. In April 2024, leadership organized a working group of inpatient stakeholders, including leadership from nursing, case management (CM), physicians, Advance Practice Providers (APP), pharmacy, rehab services as well as frontline nurses. Three key areas were prioritized for standardization and improvement: 1. Facilitation and leadership 2. Script implementation and refinement 3. Identification and escalation of barriers to care progression Facilitation and Leadership Prior to implementation, IDRs lacked ownership and consistency, with facilitation varying among charge nurses, CM, and clinical nurse leaders. The project team determined that unit CMs were best positioned to lead daily IDRs. Each inpatient unit has a triad leader model (physician, APP and RN lead), all members of the unit leadership team committed to attending rounds at least weekly to provide real-time coaching, ensure process accountability, and resolve care progression barriers. The hospital inpatient operations group also incorporated IDR oversight into its structure, designating a subset of members as IDR project owners to sustain focus and accountability. Script Standardization and Refinement Previously, only bedside nurses on some units consistently used a scripted checklist to review quality measures and care barriers. To ensure structured, efficient, and goal-oriented discussions, customized scripts were created for each role group—CM, providers, nurses, and ancillary staff. Barriers to Care Progression During IDRs providers and CM jointly identified barriers to progression, with established escalation pathways available to alert medical leadership when needed. An online survey tool was created to capture and categorize observed barriers as clinical or non-clinical, guiding targeted leadership interventions. Over the past 18 months, this survey has been refined to reflect evolving patient and system needs, supporting ongoing operational improvements.
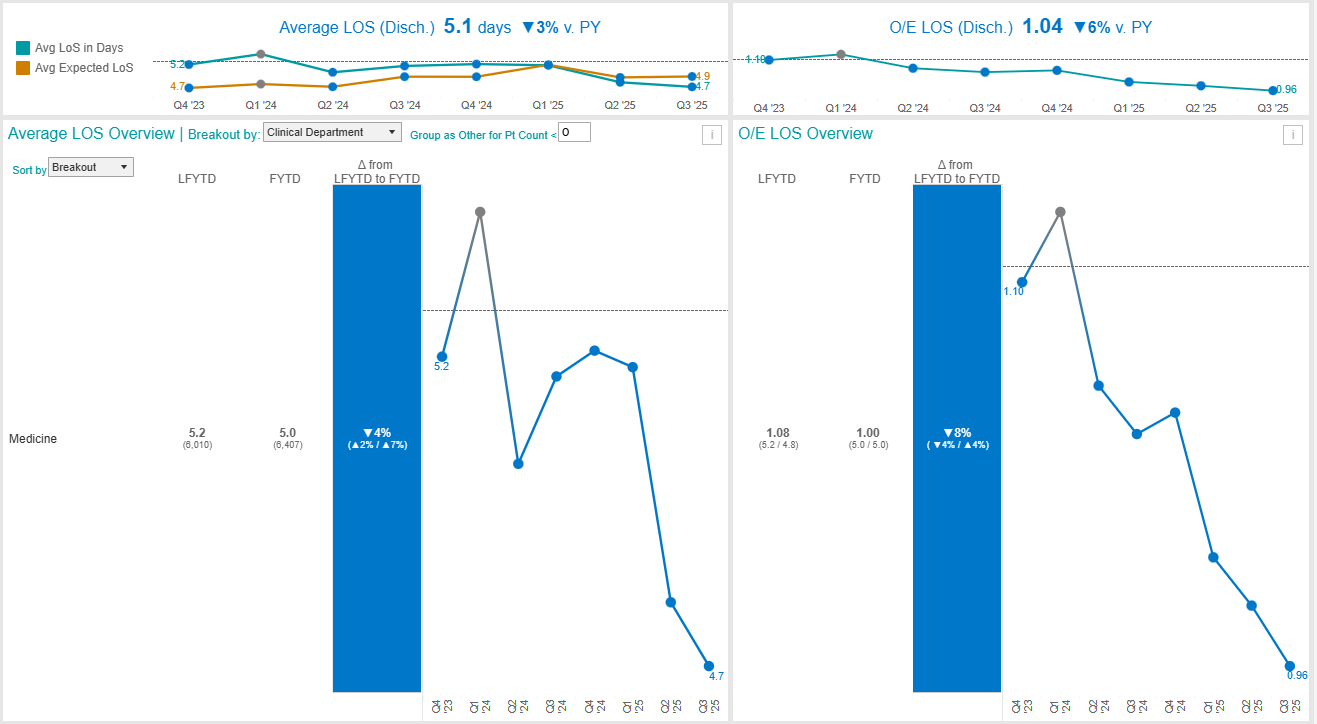
Conclusions: This initiative successfully standardized IDRs across all inpatient units and enhanced early identification of barriers to care progression. Periodic audits verify ongoing >90% adherence to scripted content across all units. Sustained engagement among staff and leaders has reinforced IDRs as a cornerstone of interdisciplinary collaboration and hospital efficiency. Since implementation, LOS at our hospital has steadily declined, with an ~ 4% reduction to date and O/E improved by ~8%. While multifactorial, these improvements highlight the impact of a structured, leadership-driven IDR process in optimizing patient flow and operational performance.