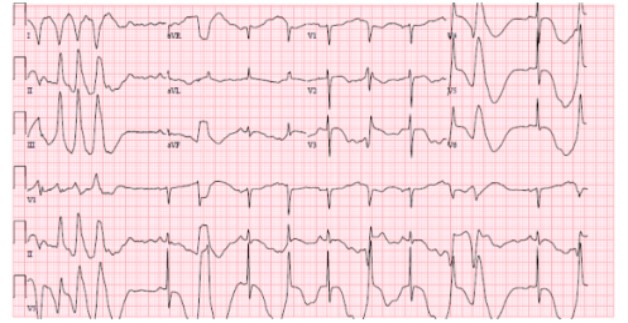
Case Presentation: A 79-year-old woman with hypertension and hyperlipidemia arrived to the ER after a syncopal episode. She was found in intermittent polymorphic ventricular tachycardia (VT). She was treated medically, briefly regaining sinus rhythm with possible ischemic changes (Figure 1). She was transferred to a cardiac catheterization capable facility. The study showed proximal left anterior descending artery narrowing of 80% leading to placement of one drug-eluting stent. Her care was continued in the cardiac ICU. She was noted to have a total cholesterol of 299 mg/dL with a calculated LDL of 215 mg/dL and started on atorvastatin 80 mg daily. She had worsening transaminitis and discharge labs were alkaline phosphatase (AP) 239 U/L, aspartate aminotransferase (AST) 44 U/L, alanine transaminase (ALT) 53 U/L. Two weeks after discharge, outpatient labs were remarkable for AST of 113 U/L, ALT of 88 U/L, and AP 423 U/L with normal bilirubin and creatinine kinase levels. Statin therapy was held and repeat blood work two weeks later showed improvement with AST of 20 U/L, ALT of 13 U/L, and AP of 215 U/L. Antinuclear antibody (ANA) and anti-mitochondrial antibody levels were negative. Drug-induced liver injury (DILI) was suspected and a PCSK9 inhibitor was initiated with no complications. After a year, she was readmitted for gastrointestinal bleeding. Due to unavailability of PSCK9 inhibitors inpatient, she was restarted on atorvastatin 80 mg daily. On her post-discharge follow-up appointment, elevated liver enzymes were once again noted. ANA was positive (1:160) with speckled pattern and anti-smooth muscle antibody (ASMA) was 1:160. Atorvastatin was held once again and repeat labs with Hepatology showed normalization of liver enzymes and decrease of ASMA level to 1:40.
Discussion: Landmark trials including the MIRACL study demonstrated the benefits of treatment with atorvastatin 80 mg daily after acute coronary syndrome. Use of high dose statins has been associated with increased risk of adverse reactions. Providers must be aware of myopathies, gastrointestinal symptoms, drug induced liver injury, and rarely statin induced autoantibodies. Statin induced transaminitis typically causes greater increase in AST compared to ALT, as seen in this case. The overall risk of DILI with statin use is estimated to be 1 in 100,000. Per the literature, there is difficulty in differentiating DILI with positive ASMA from autoimmune hepatitis (AIH) revealed by statin use given their similar antibody profiles and differences in clinical management. DILI is typically treated with removal of the offending medication with steroids sometimes used in refractory cases although with unproven benefit, while AIH involves early initiation of steroids and sometimes other immunosuppressive agents. Studies suggest that AIH may present with higher concentrations of IgG autoantibodies concentrations while DILI may have higher IgM autoantibodies. The key finding of elevated ASMA on statin reinitiation was important to solidify DILI as a concrete diagnosis and avoid long-term complications.
Conclusions: This case presentation highlights the importance of being cognizant of medication side effects. Recognition and removal of atorvastatin allowed ASMA levels and liver enzymes to normalize while preventing long-term damage. The spectrum of antibody-associated DILI and AIH in relation to statins must be further investigated to ensure proper clinical management.