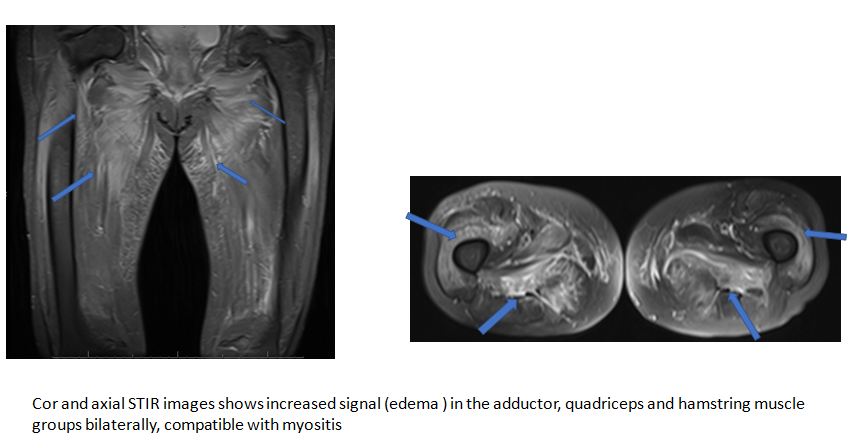
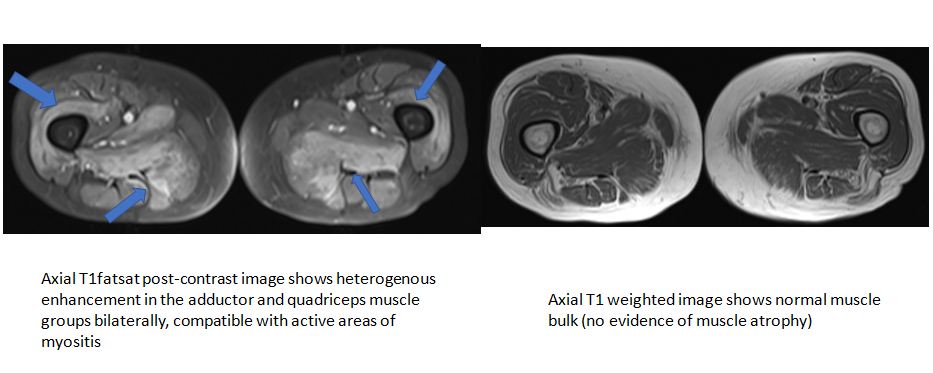
Case Presentation: A 70-year-old female with a past medical history of diabetes mellitus type 2, hyperlipidemia, hypothyroidism and GERD presented to emergency department with complaints of weakness and myalgia. The patient reported that she was having trouble dressing and walking upstairs for 2 weeks. She stated that 2 weeks ago she felt weak and fell while playing with her grandson, and the weakness gradually got worse since then. The patient also reported low back pain and proximal muscle pain that was exacerbated with moving extremities. The patient stated that she had been on Atorvastatin for several years. Initially, she was on Atorvastatin 10mg daily and 2 years ago the dose was increased to 40mg daily. On physical examination, muscle strength was 4/5 in BUE and 3/5 in BLE and sensation was grossly intact. Labs were significant for creatine kinase (CK) of 10618 U/L, troponin 287 U/L, and ALT 535 U/L, AST 537 U/L. EKG and chest x-ray were unremarkable. The patient was diagnosed with rhabdomyolysis. Elevated troponin and LFTs were secondary to rhabdomyolysis. She was admitted to the hospital, and started on aggressive IV hydration. Atorvastatin was on hold. However, CK level remains elevated despite IV hydration. Autoimmune Statin induced myonecrosis was suspected, and lab tests for myositis panel, SSA/SSB, complement levels, Vitamin D level, and HMG-CoA Reductase Ab (HMGCR Ab) were sent. The rheumatologist evaluated the patient, and she was started on high dose prednisone pending lab results. MRI of thigh muscles revealed nonspecific myositis in the pelvic and bilateral thigh musculature. HMGCR Ab came back positive 280 CU (reference range < 20CU). A muscle biopsy was also done and demonstrated myopathic changes with necrotic fibers. The patient was diagnosed with Statin Induced Autoimmune Necrotizing Myopathy (SIANM). With steroid, some symptomatic improvement was noted and the patient was discharged on steroid with outpatient follow-up with the rheumatologist. At the outpatient follow-up, she did complain of persistent symptoms of weakness along with persistently elevated CK. The patient was then started on Azathioprine while continuing Prednisone. Her symptoms markedly improved along with the normalization of her CK level. Prednisone was gradually tapered off and the patient remains on Azathioprine.
Discussion: Statins are one of the most widely prescribed drugs around the globe. Statins have a spectrum of muscular side effects that includes myalgia, myopathy, myositis, myonecrosis, and rhabdomyolysis. Statin-induced necrotizing autoimmune myopathy (SIANM) is the most severe form of skeletal muscle related side effect. In SIANM, muscle weakness progresses even after cessation of statin therapy. SIANM should be considered in a patient on statin therapy who develops proximal muscle weakness along with markedly elevated CK. To diagnose SIANM, along with elevated CK, HMGCR Ab test, a muscle biopsy and an MRI of skeletal muscle can be considered. Patients are usually started on high dose corticosteroids and/or IVIG initially. In many cases, patients also need additional immunosuppressive drugs. Tapering off medication can be challenging sometimes since the withdrawal of immunosuppressive drugs sometimes can lead to the recurrence of the disease.
Conclusions: The physician should have a high index of suspicion for SIANM in a patient on statin who presents with muscle weakness and elevated CK level. So that early diagnosis, cessation of statin, and initiation of immunosuppressive drugs can be done in time.