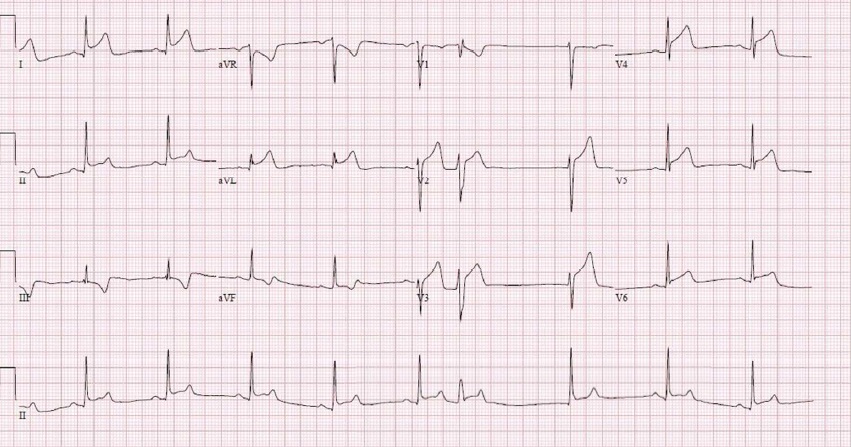
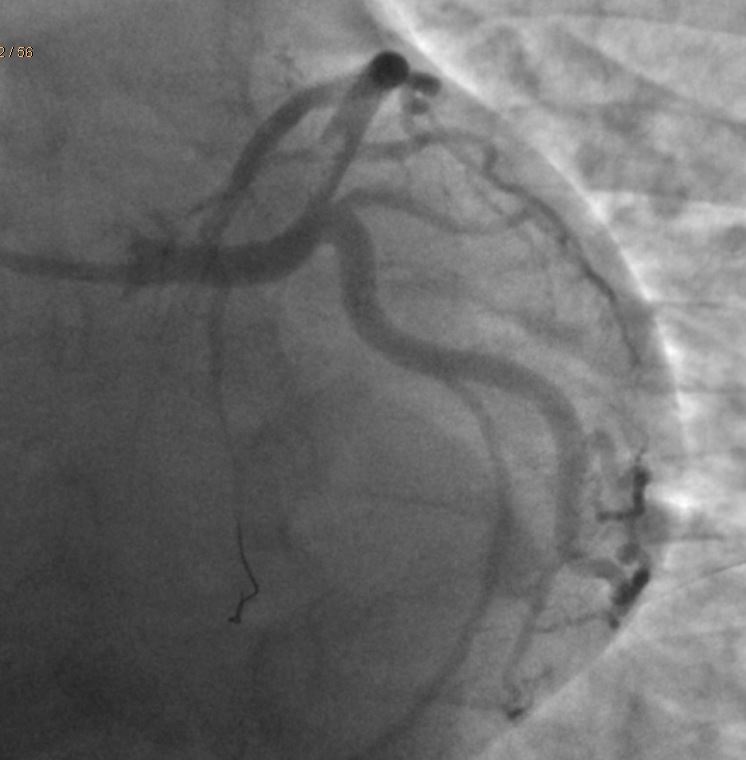
Case Presentation: A twenty-two-year-old male with no significant past medical history who presented with chest pain and found to have ST-segment elevation in leads II, III, aVF and V4-V6 leads. On subsequent EKG’s, patient had new ST-segment elevations in antero-lateral leads with dynamic changes. Cardiac catheterization showed acute dissection with thrombosis of the distal left main coronary artery leading into the ostial left anterior descending artery. Patient had no cardiac risk factors including hypertension, hyperlipidemia, diabetes or family history of early cardiac disease. On further inquiry, patient was found to be on two separate performance enhancing supplements which contained Synephrin, a sympathomimetic chemical which was later attributed as the cause of his acute coronary syndrome. Synephrin acts on alpha-1 adrenergic receptors causing peripheral and coronary vasoconstriction, hypertension and hyperglycemia. Increased hemodynamic stress on the coronary arteries can lead to fatal dissections. Ours is an atypical case of synephrin-induced non-atherosclerotic spontaneous coronary artery dissection which helps caution the physicians about the importance of dietary supplement use in the history and possible side-effects of such performance enhancing additives.
Discussion: This is an interesting case of a young active male with no apparent past medical or familial risk factors who presented with STEMI secondary to dissection with thrombosis of distal left main coronary artery extending to proximal LAD. The patient’s condition could be attributed to his use of synephrin containing weight-loss and performance-enhancing supplements. Administration of beta blockers pre-procedure might also have led to the unimpeded alpha action of the adrenergics in this case. Synephrin is a naturally occurring alkaloid which has been used in combination with caffeine in several weight-loss and dietary supplements. Pharmacologically synephrin has its action on alpha-1 adrenergic receptors causing effects such as peripheral vasoconstriction, hypertension and hyperglycemia. Unsupervised use of such supplements could be risky and even fatal. A definitive causal relation between the dietary supplement intake and coronary dissection cannot be drawn in this case; however, given the paucity of any other likely risk factors, the event is presumably secondary to the hypertension and sympathetic over -activity from synephrin.
Conclusions: Adding sympathomimetic chemicals like ephedra-containing compounds are highly effective in performance enhancement with the potential of causing fatal side cardiac and respiratory side effects. Ephedra containing compounds were banned by the FDA. However, this has led to the use of alternative sympathomimetic compounds like synephrin in these dietary supplements. Dietary supplement and weight loss reduction drug industries are highly lucrative and the unscrupulous and potentially dangerous practice of adding sympathomimetic compounds for quick results is rampant. More FDA regulations have to be implemented in this regard for the safety of the users. For any such patients presenting with acute coronary syndrome, use of beta blockers should be avoided. Furthermore, it is important for physicians to be cognizant of sympathomimetics in the dietary supplements and elicit such history in atypical cases such as the one presented here in order to avoid diagnostic confusion and inadvertent harm to the patient.