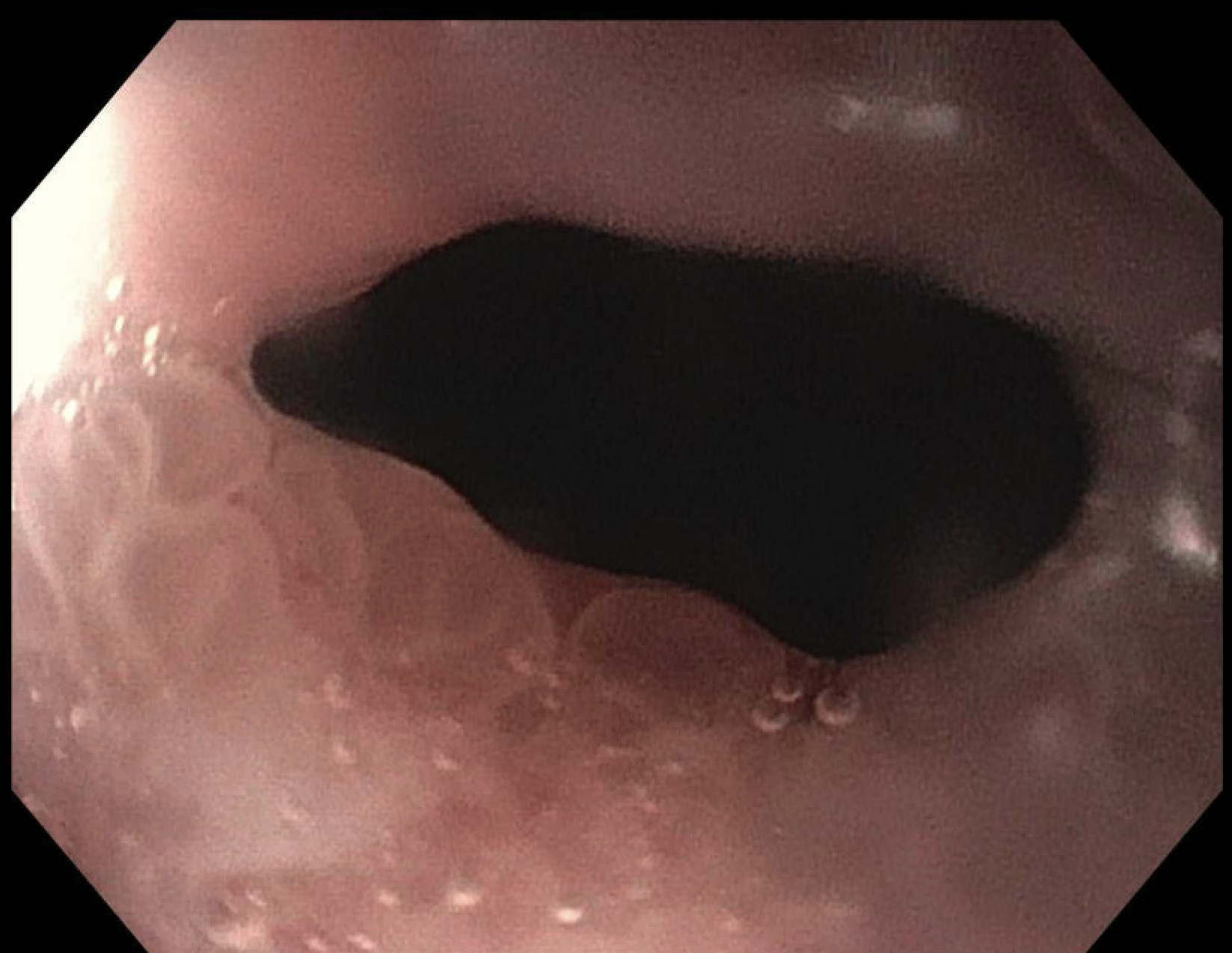
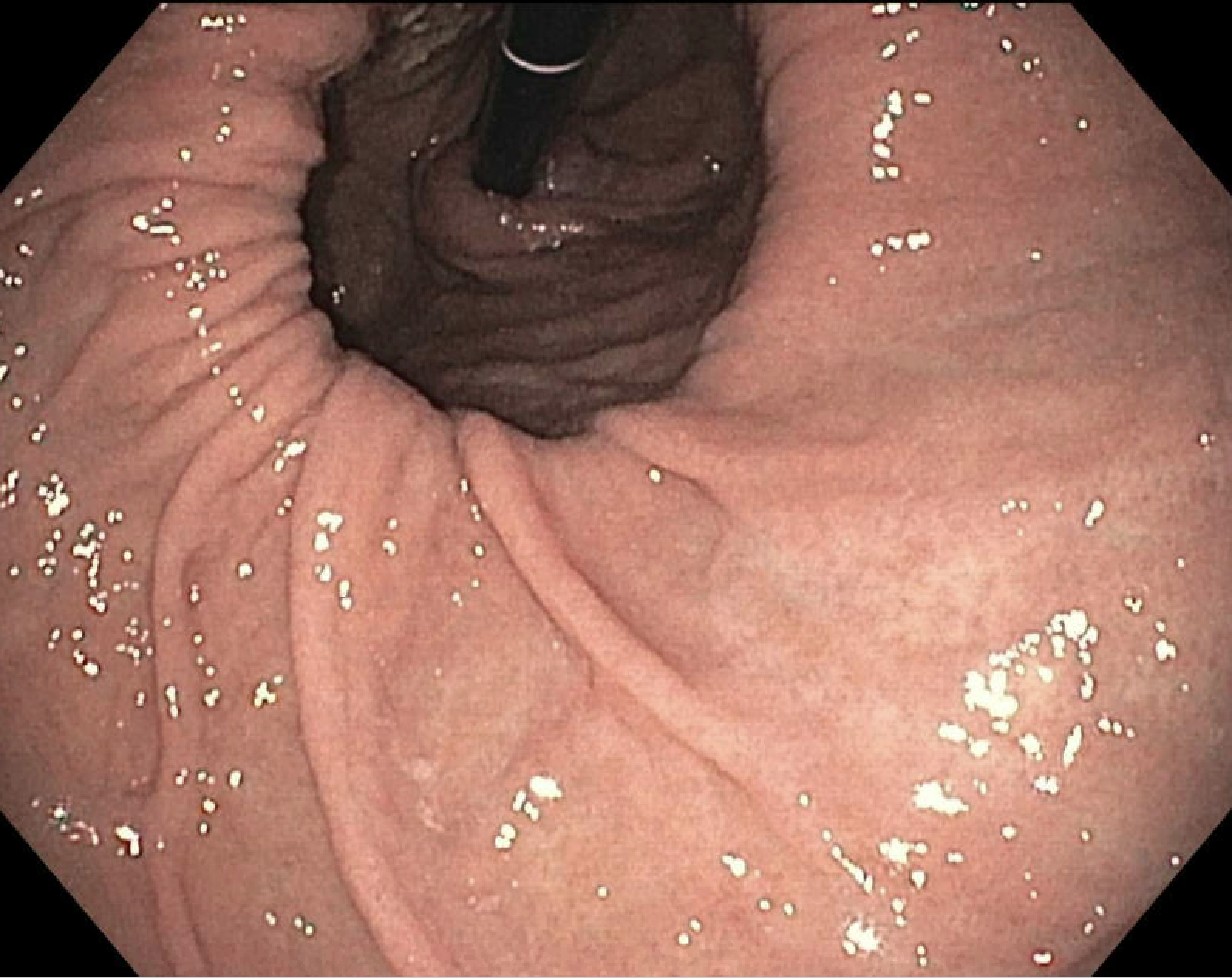
Case Presentation: A 75-year-old female with a history of gastrointestinal bleeding from a duodenal ulcer and post-transfusion hepatitis C presented to an outside hospital with generalized weakness, intermittent epigastric discomfort, and two weeks of melena. She denied NSAID or steroid use. She has been a bloodless patient since acquiring hepatitis C. On examination, the patient had stable vital signs but appeared pale. The rest of the exam was unremarkable. Her initial hemoglobin was 6.1 g/dL, dropping to 4.9 g/dL after fluid resuscitation. Reticulocyte count was 5.07%, with a corrected value of 2.1%. Iron panel showed a TSAT of 10%, with no other evidence of iron deficiency. CT angiogram of the abdomen and pelvis did not show acute hemorrhage but revealed a large hiatal hernia. The patient was started on IV iron, vitamin B12, and folic acid and transferred to our center for further bloodless management on day 6 of admission. Upon arrival, she was hemodynamically stable, but her hemoglobin was 4.7 g/dL. The bloodless management protocol was initiated along with involvement of the Patient Blood Management (PBM) team. The protocol included subcutaneous epoetin alpha, IV iron sucrose 200 mg daily for 5 days, vitamin B12 1000 mcg once, and folic acid 1 mg daily. Additional measures included limiting blood draws to every 3 days, using smaller collection tubes, administering supplemental oxygen, restricting patient activity, and monitoring for signs of tissue hypoxia with daily electrocardiograms. She was taken for endoscopy which revealed congestion at the gastroesophageal (GE) junction, a 10 cm hiatal hernia with Cameron lesions but no other ulcers. No interventions were performed. Pathology report showed GE junctional mucosa with submucosal ischemic changes consistent with a clinical diagnosis of Cameron lesion. The patient’s hemoglobin improved to 6.9 g/dl with a corresponding increase in reticulocytes to 11.8%, corrected at 8% within 10 days. She was discharged in a stable condition to continue her supplementation and for outpatient planning for repair of the hiatal hernia.
Discussion: PBM focuses on strategies to preserve and optimize a patient’s own blood.1 It is a rapidly evolving field with three main pillars: reducing unnecessary blood loss, enhancing red blood cell production, and improving blood’s oxygen-carrying capacity2. In this case, emergent endoscopy was performed to identify the bleeding source, while limiting blood draws to every three days and using smaller collection tubes minimized blood loss. Red blood cell production was boosted through epoetin alpha, folic acid, iron, and vitamin B12 supplementation. Finally, plasma can supply up to 30% of oxygen delivery in form of dissolved oxygen by increasing the PaO3. We gave supplemental oxygen as well was minimized oxygen consumption utilization by limiting the activity of the patient. Other strategies that can be employed include the use of beta blockers, prompt control of fevers and even mechanical ventilation.
Conclusions: Careful management of bloodless patients can achieve similar clinical outcomes and even lower hospital costs compared to standard management.4 The establishment of a PBM committee at our institution enabled the creation of a bloodless protocol accessible to all physicians, facilitating early, strategic interventions to enhance patient outcomes.