Case Presentation: Sweet syndrome, or acute febrile neutrophilic dermatosis, is an inflammatory condition characterized by acute onset of tender skin lesions composed of dermal neutrophilic infiltrate. Clinical variants are based on lesion morphology. One variant, giant cellulitis-like Sweet syndrome, is characterized by giant erythematous lesions, a case of which is described here.
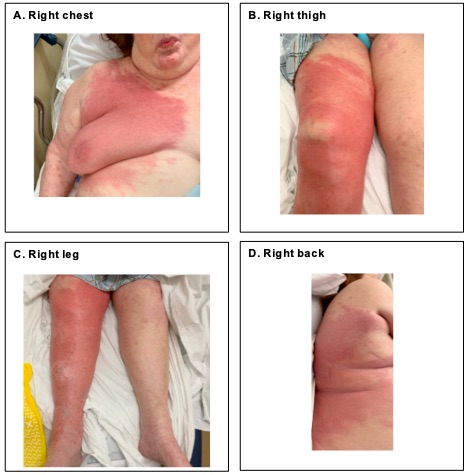
Discussion: A 90 year old woman with right breast ER/PR+ invasive ductal carcinoma s/p lumpectomy and radiation in 2014 and currently on letrozole, presented to the ED after acute onset of an erythematous rash involving the right leg, chest, face, abdomen, back, and buttocks. The rash began four days prior to presentation without pain, fevers or chills. There was no headache, neck stiffness, or sore throat. There was no skin break, insect bite, outdoor exposure, travel, new medication or skincare product, or hospitalization. On physical examination, the patient appeared well. Vital signs were normal. Skin exam revealed large erythematous, non-tender, blanching plaques. Lesions on the lower extremity, chest, and abdomen were warm, edematous, raised, and demarcated. Lesions on the face, back, and buttocks were diffuse, edematous, without clear borders (Fig 1). There were no blisters, vesicles, or drainage. Labs showed WBC 29.1 with neutrophilic predominance and ESR 78. Peripheral blood flow cytometry was normal. Blood cultures were negative. CT of the right leg demonstrated soft tissue edema without abscess. CT of the head, chest, abdomen and pelvis did not reveal mass, abscess, lymphadenopathy, organomegaly, or infectious focus. The patient was treated with cefazolin 1gm IV Q8H for non-purulent cellulitis. Lower extremity and face lesions receded while remaining lesions were unchanged. Skin biopsy revealed epidermal neutrophilic infiltrates and superficial dermal edema without leukocytoclasis, consistent with Sweet syndrome. Prednisone 80mg PO daily was initiated. The skin lesions improved swiftly. The patient was discharged in stable condition on day 7 of hospitalization.
Conclusions: Sweet syndrome is diagnosed by the acute onset of tender erythematous skin nodules or plaques with neutrophilic infiltrate and edema in the upper dermis without leukocytoclastic vasculitis. Fever, inflammatory markers, and presence of an associated infectious, inflammatory, or malignant condition support the diagnosis. This patient’s erythematous lesions with neutrophilic infiltration are consistent with the giant cellulitis-like variant of Sweet syndrome, a neutrophilic dermatosis with widespread infiltrated inflammatory plaques.Other aspects of this patient’s manifestation of Sweet syndrome are atypical. Fever, occurring in 80-90% of cases, was absent. Her lesions were nontender. Partial improvement of some lesions with antibiotic treatment suggests concomitant skin infection.The diagnosis of Sweet syndrome necessitates the search for an underlying etiology. Sweet syndrome may be idiopathic, drug-induced, or due to malignancy, infection, or inflammatory disease. Malignancy-associated Sweet syndrome may occur with new or recurrent disease. The patient’s laboratory and imaging workup revealed no evidence of hematologic or solid tumor malignancy. She requires breast imaging to evaluate for recurrent breast cancer.Clinicians should maintain familiarity with Sweet syndrome and its giant cellulitis-like variant to enable prompt diagnosis and workup for etiologic conditions.