Background: Emergency department (ED) crowding leads to prolonged boarding times, delayed admissions, and decreased operational efficiency. Level loading (LL) in a multi-hospital organization is the intentional balancing of patient volume across all hospitals in the system, rather than allowing one hospital to become overloaded while others have capacity. A clinical expeditor (CE) is a patient flow coordinator who facilitates patient flow and distribution across the hospital system. We studied the Impact of LL with the help of a CE on Key Hospital Throughput and Performance Metrics.
Purpose: We conducted a retrospective analysis of hospital throughput metrics before and after the implementation of LL with a CE at INTEGRIS Health Baptist Medical Center, which is a tertiary care and flagship hospital of INTEGRIS Health in Oklahoma City. We compared the following metrics: Percentage of patients staying in the ED longer than 2 hours after an admit order, Percentage of admitted patients with ED stay time greater than 280 minutes, Mean time from admission order to ED departure, Mean total ED length of stay (LOS) for admitted patients, trends in transfer refusal rate and trends in hospital’s Case Mix Index (CMI). We used SPSS software to perform statistical analysis to compare the means between the two groups. A p-value < 0.05 was considered statistically significant.
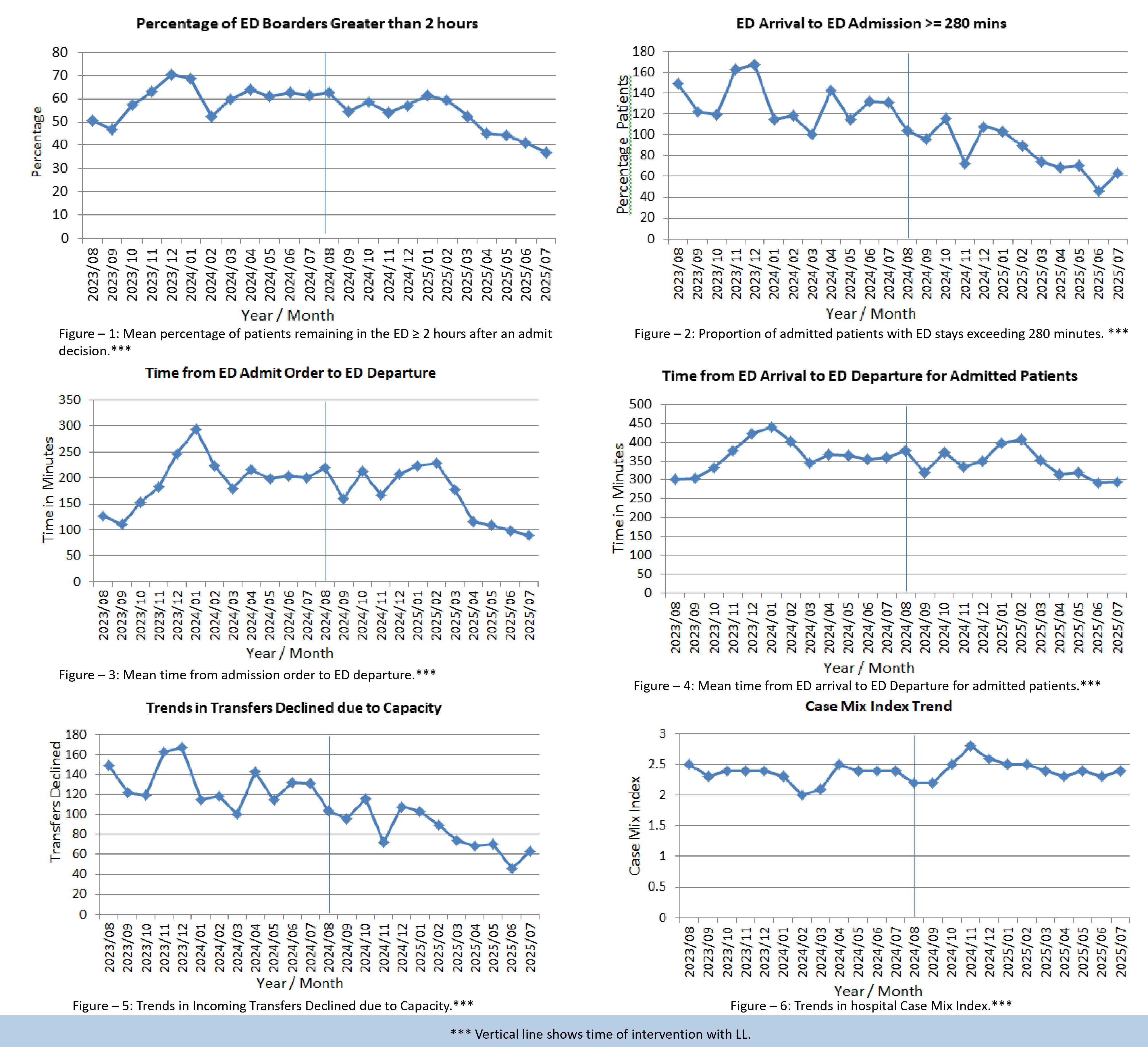
Description: Following implementation of LL with a CE, we noted a statistically significant 7.6% decrease (95% CI, 1.01–14.17; p< 0.05) in the mean percentage of patients remaining in the ED longer than 2 hours after an admit decision (Figure - 1) and a 7.1% decrease in the proportion of admitted patients requiring ED stays exceeding 280 minutes, from 68.63% to 61.47% (95% CI, 2.38–11.92; p< 0.05) (Figure - 2). We also noted a statistically significant 38.5 minutes decrease from 194.8 minutes to 156.3 minutes in the mean time from admission order to ED departure (95% CI, 2.45 - 81.78; p< 0.05) (Figure - 3) and a 38.5 minutes decrease in the total ED LOS for admitted patients, from 363.7 minutes to 335.7 minutes (95% CI, 5.70–61.77; p< 0.05) (Figure - 4). There was a statistically significant decline in incoming transfer refusals from a mean of 131 refusals per month to 84 refusals per month (95% CI, 29.73–63.82; p< 0.05) (Figure - 5), which led to a positive trend in the hospital's CMI that increased from 2.34 to 2.43 (p=0.17) (Figure - 6).
Conclusions: Our results showed that LL at a tertiary care hospital ED significantly improved ED throughput metrics by reducing boarding times and overall ED LOS for admitted patients. It improved operational efficiency and enhanced patient flow, allowing for quicker transitions from ED admission decision to inpatient bed placement. It led to better bed utilization and improved capacity management, as shown by the reduced refusals to Transfer-In requests. Improvement in the Case Mix Index showed that our tertiary care hospital got to see patients with higher acuity, potentially leading to increased reimbursement. Our results show that implementation of LL at a tertiary care hospital can serve as a scalable, system-level strategy to enhance patient flow, reduce ED congestion, and improve overall hospital throughput performance.