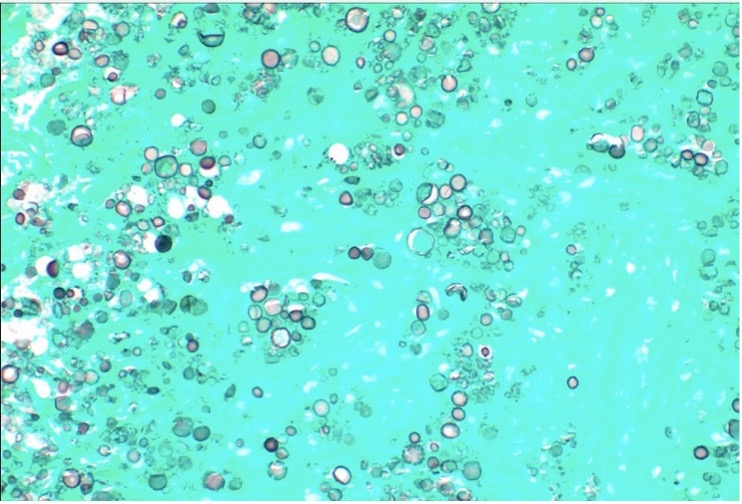
Case Presentation: A 53-year-old immunocompetent female with a history of well-controlled type 2 diabetes mellitus had incidentally found asymptomatic right lower lobe lung masses, the largest of which measured 6.5 cm x 2.4 cm. She underwent a CT-guided lung biopsy of these for further evaluation. The pathology report did not reveal a malignancy, but instead showed necrotizing granulomas with innumerable Grocott Methenamine Silver (GMS) and Mucicarmine stain positive fungal organisms. Subsequent blood testing revealed a cryptococcal antigen titer of 1:32, an absolute CD4 cell count of 1686 cells/uL with 64% CD4 Helper Cells and no detection of HIV, Histoplasma, Blastomyces, Candida, Coccidioides or Aspergillus. Review of risk factors for fungal exposure, including travel to endemic regions, spelunking, or pigeon exposure, were negative. She was initiated on fluconazole therapy and discharged home with outpatient infectious disease follow-up. As of the most recent outpatient visit, she was tolerating the fluconazole therapy without complications with plans to repeat imaging to monitor response to therapy.
Discussion: Cryptococcal infections are well known to cause disease in individuals with AIDS, neutropenia, cirrhosis, or organ transplantation; but uncommonly may present as asymptomatic lung masses in immunocompetent individuals. Thambidurai et al described pulmonary cryptococcal infections as “the great mimicker” and studies have demonstrated morphological similarities in cryptococcal lung masses and lung tumors. The IDSA recommends 6-12 months of Fluconazole therapy, with the duration guided by response to treatment. Although reports of incidentally found asymptomatic cryptococcal pulmonary infections in immunocompetent individuals have demonstrated radiographic improvement with observation alone, fluconazole therapy is curative and decreases risk of symptomatic systemic dissemination.
Conclusions: This case demonstrates the importance of keeping a broad differential diagnosis when investigating pulmonary masses, including tumors, bacterial and fungal pathogens. Although a malignancy is the more common and feared diagnosis of pulmonary masses, clinicians and radiologists should be familiar with other rare and unusual aetiologies.