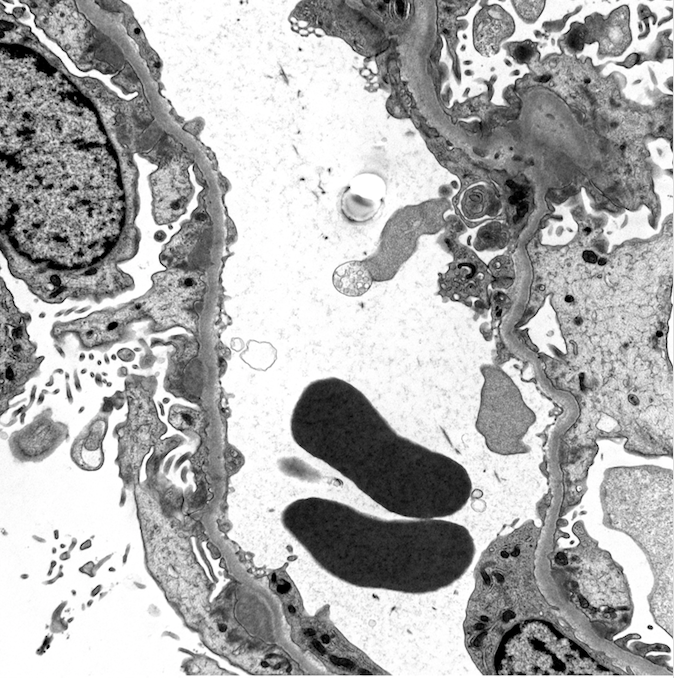
Case Presentation: A 36- year-old female with asthma presented with worsening anasarca, malaise, headache, and subjective cognitive decline over three weeks. She had been to numerous hospitals and clinics for her symptoms. Despite various treatments, including Ciprofloxacin for presumed UTI, her symptoms continued to progress. A urinalysis at an outside hospital showed 4+ protein. On presentation to our hospital, notable labs showed Creatinine of 1.28 mg/dL, BUN of 14 mg/dL, and albumin of 1.5 g/dL. 24-Hour Urine Analysis revealed sub-nephrotic range proteinuria of 368 mg/dL. Additional evaluation for autoimmune and infectious etiologies, including Hepatitis, HIV, ESR, CRP, ANA, anti-PLA2R IgG, and C3/C4, were normal. Treponemal antibody testing was positive with RPR titer of 1:16. Lumbar puncture ruled out neurosyphilis. An image-guided kidney biopsy revealed histologic patterns characteristic of membranous glomerulonephritis with a “full house” pattern on immunofluorescence staining. The patient was diagnosed with membranous nephropathy secondary to syphilis. She received intramuscular Penicillin G and Lasix treatment and was discharged on low-dose Losartan. On two week follow-up, the patient had drastic improvement of proteinuria and hypoalbuminemia to normal ranges, illustrating the potentially transient course of this disease given appropriate treatment.
Discussion: Syphilis poses a unique challenge to physicians across the US. After reaching an all-time low in cases in early 2000s, syphilis cases have increased yearly since 2001, with 41,000 new cases in 2020. Given the increasing prevalence of this highly treatable disease, it is critical to recognize the myriad clinical presentations. Syphilis can manifest in the kidneys in multiple ways, including glomerular, tubular, and vascular pathologies. Here we present a case of membranous glomerulonephritis secondary to syphilis. While many other causes of glomerulonephritis, such as autoimmune disease, require immunosuppressive medications and may progress to require renal replacement therapy, syphilis provides a typically reversible pathology which can be treated with three weekly doses of penicillin G. Co-infection with other causes of glomerular diseases, such as HIV and Hepatitis B and C is not uncommon and can make the true etiology of the glomerulonephritis challenging to determine.
Conclusions: Syphilis re-emergence requires clinicians to recognize the various manifestations of this disease, more so for vague presentations. In this case report, we raise awareness for the early diagnosis and treatment of syphilis, potentially reversing end-organ damage.