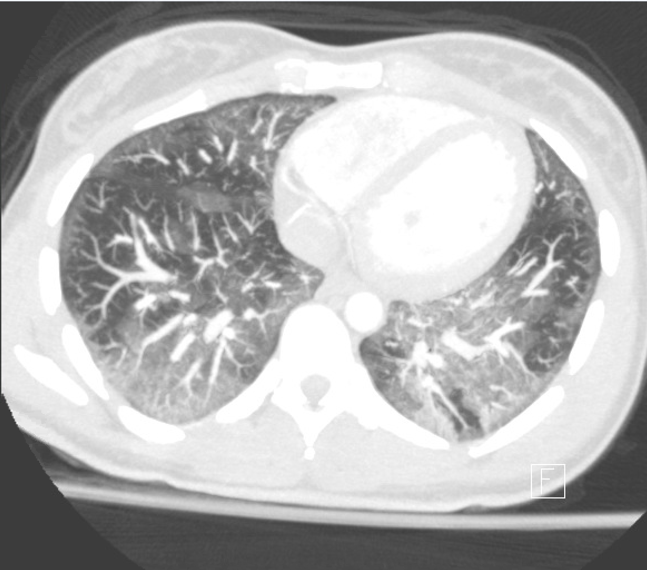
Case Presentation: A 25-year-old female with no significant past medical history presented to the emergency room with chest pain and shortness of breath. She was febrile to 40 degrees Celsius and tachypneic. Physical exam was notable for bilateral crackles in her lower bases. Her social history indicated former marijuana use and current e-cigarette use (Juule, 1 cartridge a day). She denied any other drug use and had no occupational or residential exposures. Diagnostic tests were notable for a WBC of 25 and a CT Chest that was negative for pulmonary embolism, but had lower lobe predominate ground glass opacities with septal thickening. She was admitted to the general medicine with ceftriaxone and azithromycin for presumed community acquired pneumonia. On hospital day 2, she was persistently febrile and developed an oxygen requirement. She was transferred to the Medical ICU for intubation and bronchoscopy. Bronchoscopy workup was negative including fungal and bacterial cultures. Additional workup including respiratory virus panel, CMV, HIV, ANA, ANCA, rheumatoid factor, CCP and immunoglobin panel were unrevealing. She was treated with high dose steroids and extubated two days later. Her pulmonary symptoms and fevers resolved by the time of discharge. She was discharged with a prednisone taper and counseled to stop all marijuana and e-cigarette use.
Discussion: Acute respiratory distress has been associated with e-cigarette use, prompting a Centers for Disease Control (CDC) investigation of over 450 cases to characterize vaping-induced lung injury. E-cigarettes are devices that aerosolize a liquid for inhalation by applying high heat. These liquids contain nicotine, flavoring compounds, or THC as well as contaminates such as ultra-fine particles and heavy metals. Surveys demonstrate an increase in vaping with 15.3% of adults having used an e-cigarette at least once. Cases have included a variety of pneumonitis patterns, potentially representative of different injury mechanisms. These patterns include acute eosinophilic pneumonitis, acute respiratory distress syndrome, diffuse alveolar hemorrhage, and giant cell interstitial pneumonitis. The patterns above are associated with alveolar inflammation, edema, and hypoxemia.
Conclusions: As e-cigarette usage increases there will likely be a rise in vaping-induced lung injury. A detailed social history including type of device and liquid compounds is important as the component responsible for lung injury is currently unknown.