Case Presentation: A 69-year-old African American woman with diabetes mellitus, a chronic indwelling urinary catheter, recurrent catheter-associated UTIs, bedridden status, and an infected sacral ulcer presented with acute altered mental status. She was hypotensive and tachycardic. Laboratory evaluation showed leukocytosis, severe anemia, hypoglycemia, and markedly elevated procalcitonin. A Pelvic CT confirmed sacral osteomyelitis with associated abscesses. She was admitted to the ICU in septic shock and started on vasopressors, fluid resuscitation, and broad-spectrum antibiotics. Her recent hospitalizations for urosepsis included prior blood cultures growing Escherichia coli and Proteus vulgaris. During this admission, blood cultures again yielded Proteus vulgaris on multiple draws. Transthoracic echocardiography demonstrated an 8-mm vegetation on the noncoronary cusp of the aortic valve, confirming native valve IE. Antimicrobial therapy was adjusted to carbapenem-based coverage guided by sensitivities showing multidrug resistance.
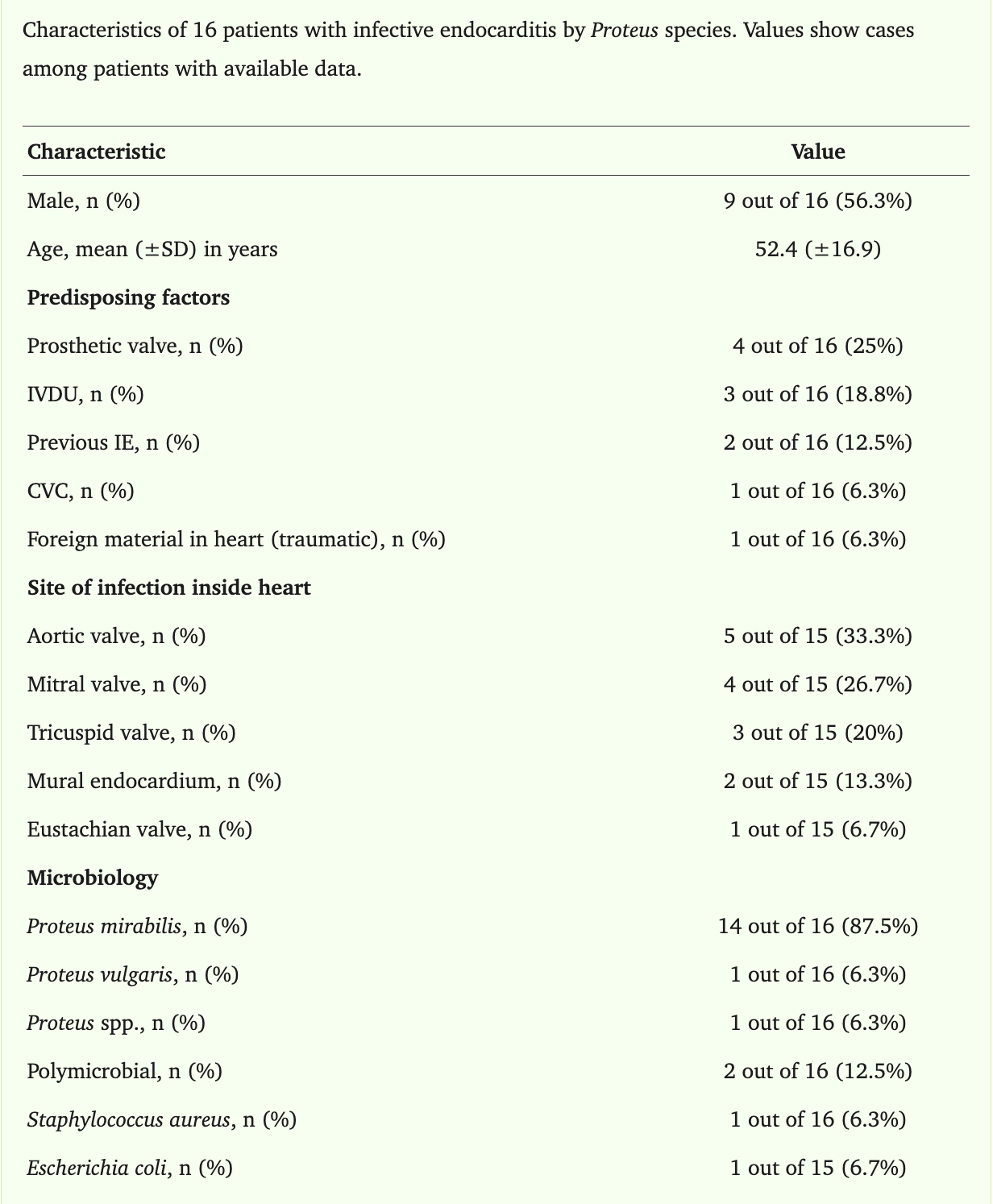
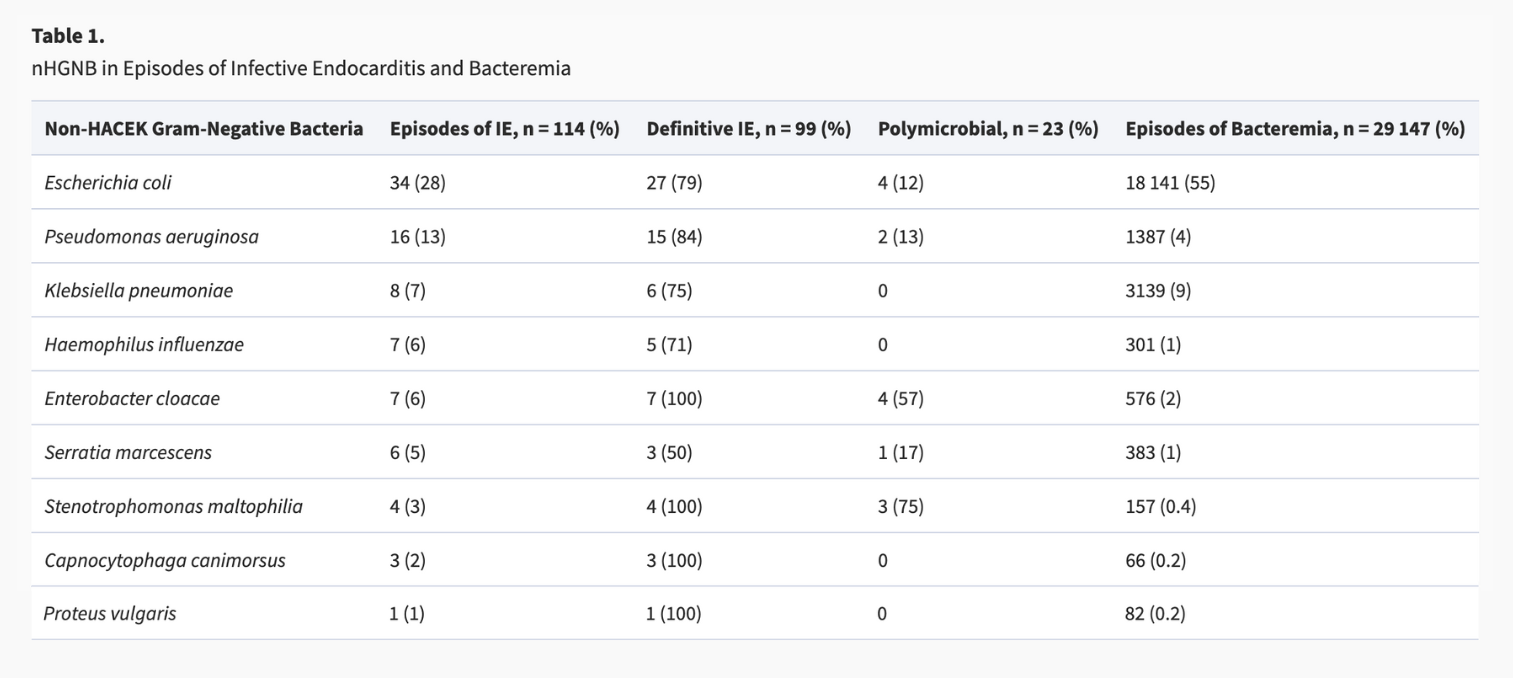
Discussion: Infective endocarditis (IE) is a life-threatening infection of the endocardial surface of the heart, most commonly caused by Staphylococcus aureus (31.2%) and viridans group streptococci (16.6%). The annual incidence in the United States is approximately 12.7 per 100,000 persons, with the mitral (41.1%) and aortic (37.6%) valves most often affected. Gram-negative pathogens account for fewer than 5% of IE cases, and Proteus species represent < 1%, with most involving P. mirabilis. Proteus vulgaris endocarditis is exceedingly rare, with fewer than 20 published cases.
Conclusions: Proteus endocarditis is thought to result from bacteremic seeding in patients with chronic urinary tract colonization or catheter use. While UTIs are a common cause of Gram-negative bacteremia, progression to IE is rare. Gram-negative IE carries reported mortality rates of 21–43%, partly due to delays in recognition, antibiotic resistance, and limited evidence to guide management. Surgical intervention is often required, yet recommendations for optimal antimicrobial duration remain unclear because available data are limited to case reports and small series. This case highlights the importance of considering IE in patients with persistent Gram-negative bacteremia, particularly those with long-term catheters or a history of recurrent UTIs. Early echocardiography and timely adjustment of antimicrobial therapy are essential. As chronically catheterized and medically complex populations continue to grow, further research is needed to clarify treatment strategies for rare pathogens, such as Proteus vulgaris.