Background: Adults with sickle cell disease (SCD) often present with extremely painful acute vaso-occlusive crises (VOC). VOC guidelines encourage early initiation of opioids, but are lacking in a standardized approach to achieve adequate analgesia and subsequent de-escalation. Various SCD studies comparing continuous basal versus demand bolus patient-controlled analgesia (PCA) show conflicting outcomes. Thus the objective of our pilot was to develop a standardized approach to pain management utilizing PCA and a Tiered Oral Therapy Protocol (TOTP) in an effort to affect healthcare utilization by decreasing length of stay without increasing readmission rates.
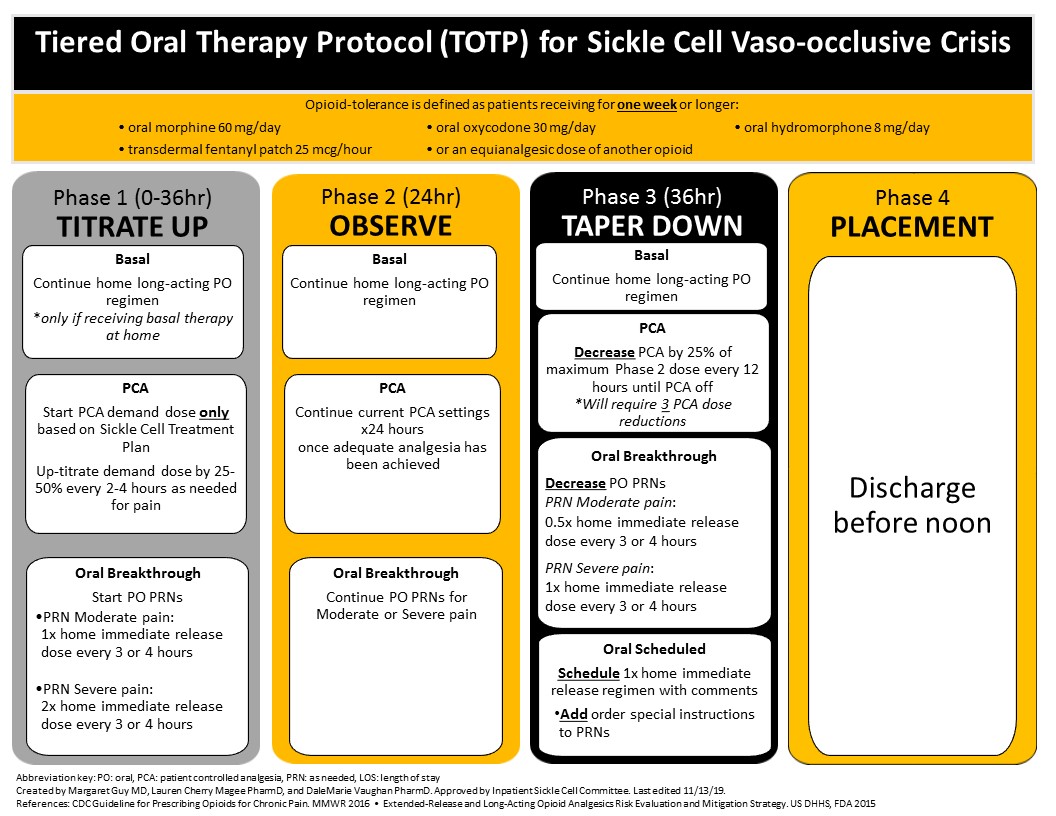
Methods: We studied admissions of 31 SCD (any genotype) patients (8 males, 23 females) ≥ 18 years old, all African-American, admitted for VOC, and treated by hospitalist providers using TOTP on one medical unit at an urban academic medical center from July 2018 to June 2019. Inpatient admissions for one calendar year prior to the initial TOTP admission served as the patient’s historical controls. TOTP is guided by the patient’s individualized treatment plan and starts with continuation of their home basal dosing, demand dose only PCA, and immediate-release oral opioids for additional breakthrough pain. The initial goal is aggressive up-titration of opioids until adequate analgesia. After a period of stability the next phase encourages timely, aggressive down-titration of opioids to speed discharge. We primarily compared length of stay (LOS), hospital charges, and 30-day readmission rates for TOTP vs historical controls. Secondarily, we compared total morphine milligram equivalents (MMEs) and adverse safety events: opioid-related rapid responses, naloxone administration, or falls.
Results: Utilization of TOTP resulted in reductions in LOS (21%, 4.7 days controls vs. 3.7 days TOTP, p<0.014), and hospital charges ($1,627,497.73 controls vs. $944,528.96 TOTP, p=0.1403), and an insignificant increase in the 30-day readmission rate (35.6% controls vs. 42.7% TOTP, p=0.5027). Hospital charge data is difficult to interpret as a full year of post TOTP encounters are not available for all patients. Overall there was a reduction in total MME administered during the inpatient admission: 361,824 MME pre-TOTP vs. 255,036 MME post-TOTP. Additionally, there were no TOTP vs. historical control differences in opioid-related safety events.
Conclusions: Standardization of therapy using the TOTP improved length of stay and reduced charges for patients with sickle cell disease admitted for acute VOC without increasing adverse safety events or significantly impacting the 30 day readmission rate. We have enlarged this pilot to include other medical units to test whether we can reproduce our initial one-unit success. As TOTP was but one among several interventions in an Adult SCD Medical Home additional testing in other hospitals is necessary to exclude confounders.