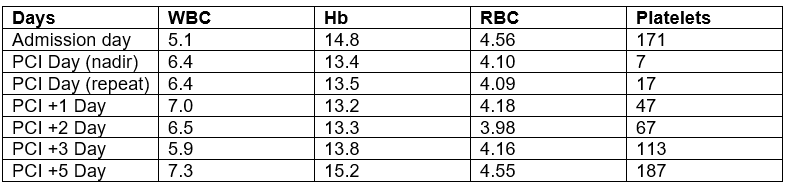
Case Presentation: We present a case of a 50-year-old male with a history of lateral and inferior wall myocardial infarctions (MI), who was admitted with complaints of shortness of breath and chest pain that had progressively worsened over the past three days. MI was suspected, but the EKG showed no acute changes, and serial troponins were negative. Complete blood count (CBC) and comprehensive metabolic panel were unremarkable. On the third day of admission, the patient’s chest pain and shortness of breath worsened, and repeat troponins were elevated (275 ng/L). CBC showed Hb of 14.8 gm/dL, WBC 5.1×10^3/mcL, and platelets of 171×10^3/mcL. The patient received a bolus of Aggrastat (Tirofiban), underwent LHC, and was found to have 70%-80% in-stent stenosis in the mid-segment of LAD with TIMI-3 flow. A drug-eluting stent was placed. Post-procedure, he was started on tirofiban infusion. The patient was clinically stable but developed post-procedural hypotension and gum bleeding. Repeat ECG and TTE were unremarkable, with a normal ejection fraction, and no pericardial effusion was found. Repeat CBC showed that his platelets had dropped to 7×10^3/mcL with stable Hb (13.4 gm/dL). CBC was repeated to rule out any artifacts. A repeat CBC showed a platelet count of 8 x 10^9/mcL. Tirofiban was stopped. Patient’s peripheral smear showed an absence of platelets. He was given a stat dose of dexamethasone 20 mg IV. Repeat platelet counts six hours later were 17 x 10^3/mcL, followed by improvement to 47 x 10^3/mcL and 113 x 10^3/mcL on the second and fourth days post-procedure. The patient tested negative for HBV, HCV, HIV, and H. pylori infection to rule out other causes of thrombocytopenia. Platelet count continued to improve; on day 6 post-procedure, platelet count was 187×10^3/mcL.
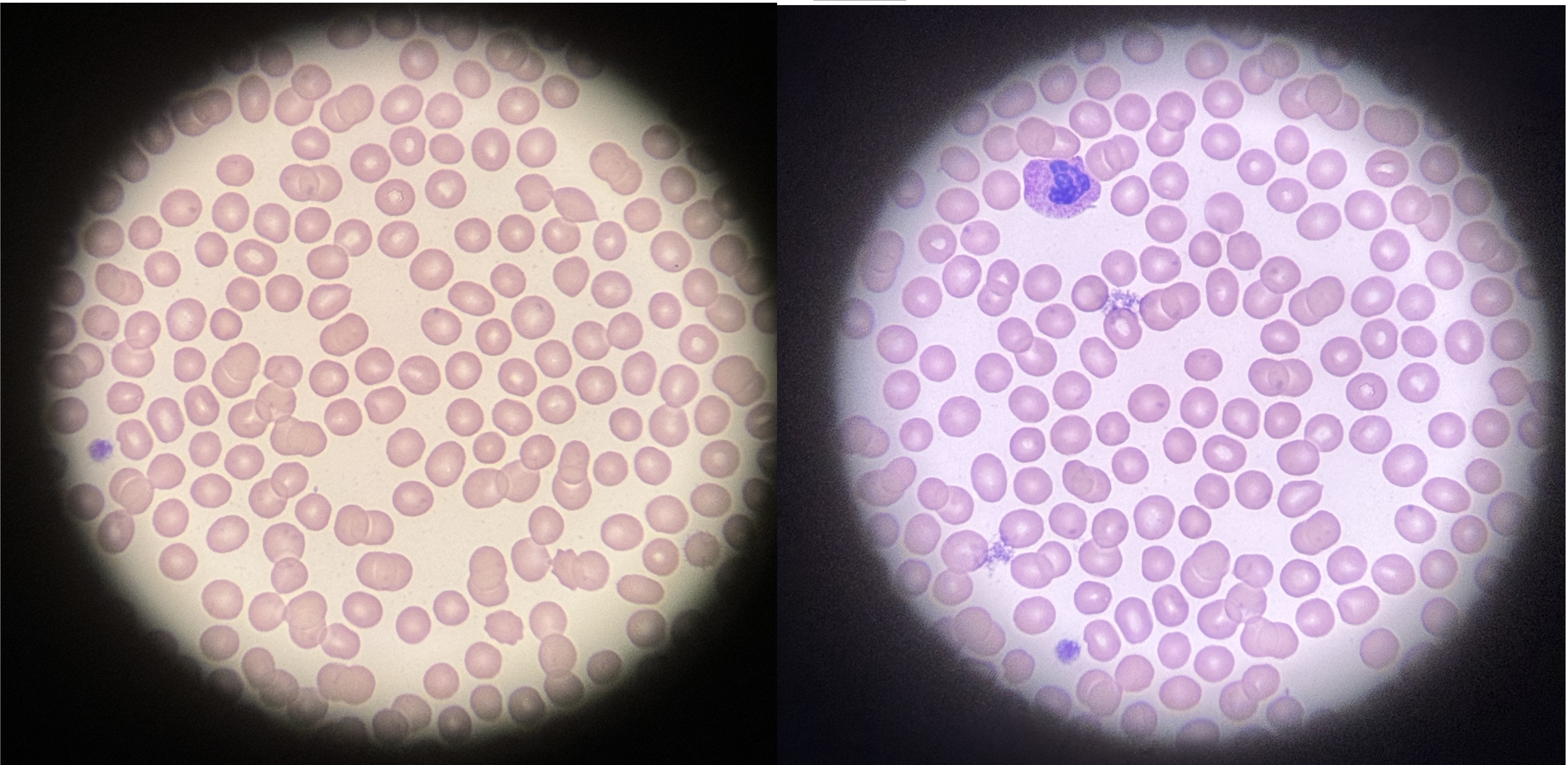
Discussion: Left heart catheterization (LHC) can serve as a diagnostic as well as a therapeutic procedure. In patients who are found to have reduced coronary blood flow can be stented to improve coronary circulation. Patients undergoing LHC receive antiplatelet agents, including Tirofiban, a glycoprotein IIb/IIIa receptor blocker, to prevent the formation of blood clots. It is a very safe drug but has a severe and very uncommon side effect of thrombocytopenia. This case highlights a very rare and severe side effect of tirofiban use. Acute severe thrombocytopenia (< 10x10^3/mcL) can occur < 12 hr after Tirofiabn administration. It is a rare but severe adverse effect that requires prompt discontinuation of the drug. Drug-induced thrombocytopenia is the diagnosis of exclusion, and other causes such as concomitant hepatitis and HIV infections should be ruled out. Visualization of the peripheral smear will rule out pseudo-thrombocytopenia due to platelet clumping.
Conclusions: Patients receiving Tirofiban should have their platelets monitored before, 2-hr, and 6-hr post-drug administration for early identification. Drug discontinuation, steroid administration, and supportive management are cornerstones of treatment, which can be supplemented with platelet and IgG administration when needed. Patients who develop thrombocytopenia should avoid the use of Tirofiban indefinitely