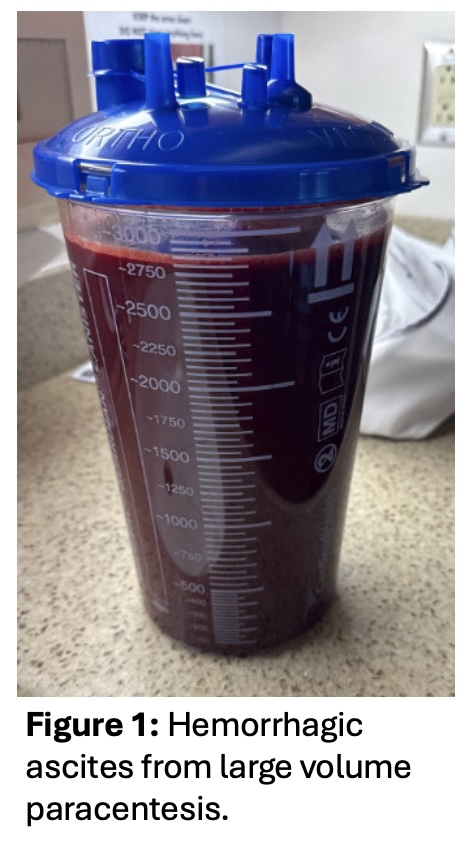
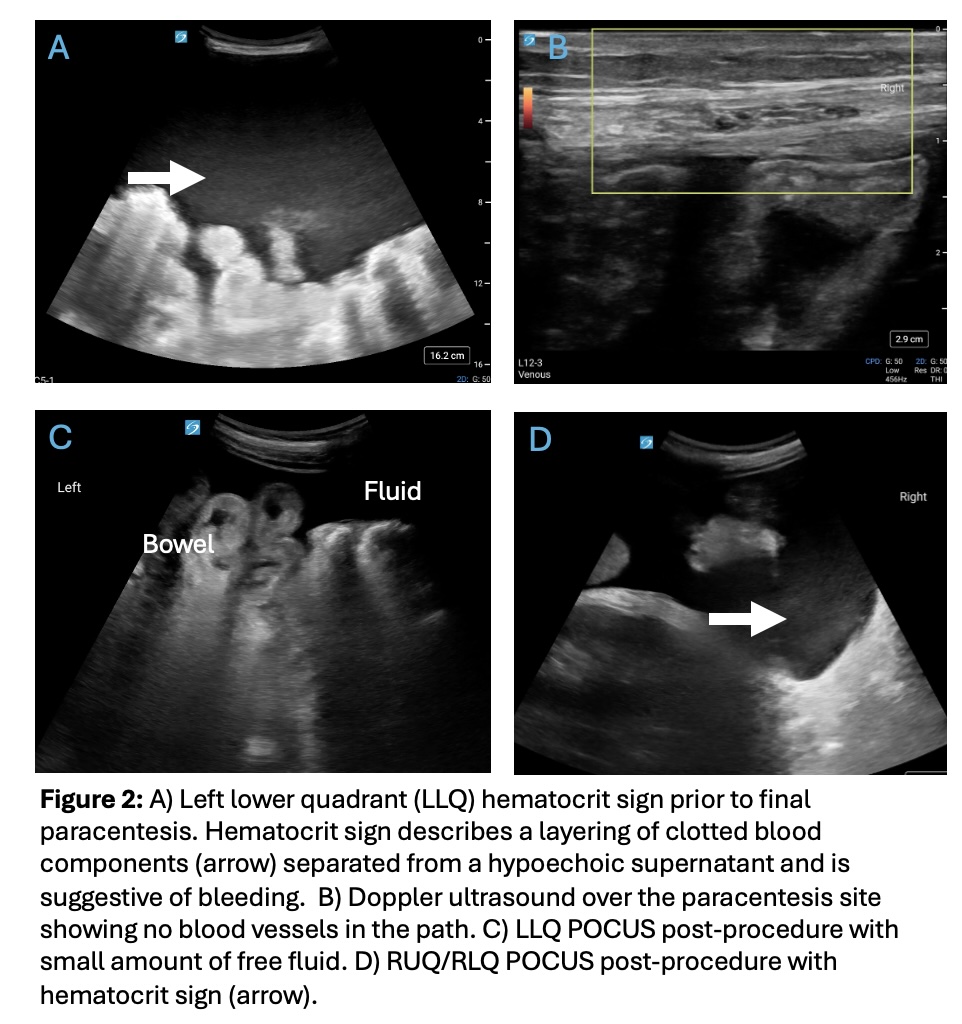
Case Presentation: A 34yo with alcohol-induced cirrhosis presented with fatigue. She had a hemoglobin (Hb) of 5.3g/dl, creatinine 3.43mg/dl (baseline 0.5), and total bilirubin 20.4mg/dl with a MELD of 40. Workup showed no GI bleeding. Large volume paracentesis (LVP) was performed with clear yellow fluid removed and no evidence of spontaneous bacterial peritonitis. She was transferred to our hospital for transplant evaluation.On admission, an LVP in the right lower quadrant (RLQ) yielded 5L of bloody ascites. Hb dropped from 7.7 to 5.4g/dl; CTA abdomen did not show active extravasation, but the team suspected possible vessel injury. Hb hovered around 7g/dl after transfusions. LVP ~10 days later in the LLQ removed 11 liters of bloody ascites (Fig 1). Hb decreased from 7.3 to 5.6g/dL. Point-of-care ultrasound (POCUS) did not reveal any blood vessels in the needle path and trace fluid on the left, though showed a “hematocrit sign” in the RUQ, which had been seen prior to the procedure and had been attributed to old bleeding (Fig 2). Repeat CTA showed “subtle area of contrast extravasation in the LLQ concerning for active hemorrhage.” Angiogram showed a small pseudoaneurysm off a branch of the inferior epigastric artery (IEA). Prophylactic embolization of the L deep circumflex and IEA was performed. Despite this, Hb continued to decline and she developed renal failure. She was started on dialysis and underwent transplant that evening. The operation showed active bleeding from the gallbladder with adjacent adhesions which avulsed the liver capsule, corresponding to the source of hemorrhage. The LLQ and inferior epigastric vessels showed no evidence of damage or recent hemorrhage.
Discussion: Hemorrhage is a rare complication of LVP. Direct injury to abdominal wall vessels can cause significant bleeding. Alternatively, increased pressure from ascites may tamponade varices at risk for bleeding such that the rapid drop in pressure that accompanies an LVP may predispose to bleeding. Regardless of cause, bleeding can be severe, leading to the need for transfusions, acute renal failure, and clinical instability. Surgery or embolization are often required.We suspect our patient bled from her gallbladder due to liver disease and coagulopathy, which has been reported in the literature. Bleeding was temporarily slowed by pressure from the ascites, but when the ascites was removed, the rapid decrease in intraabdominal pressure resulted in hemorrhage. At our hospital, ultrasound is used to improve paracentesis safety and success by identification of a fluid pocket and assessment of the proposed needle path for blood vessels. Despite best practices, there are other rare causes of hemorrhage that can be life-threatening.This case highlights the importance of avoiding premature closure. While vessel injury was a possible cause of our patient’s Hb drop, there was evidence pointing towards another etiology (lack of visible vessels at the insertion site, hematocrit sign in the RLQ, 2 episodes of bleeding after paracentesis at different sites, and continued Hb drop despite embolization). The source of bleeding was identified due to the patient’s emergent liver transplant, but may have been delayed further if she did not have an operation.
Conclusions: This case highlights the importance of recognizing how fluid removal may indirectly lead to hemorrhage after LVP. Awareness of this mechanism allows for vigilance in patients who may be at risk for serious bleeding and can expedite diagnosis and management.