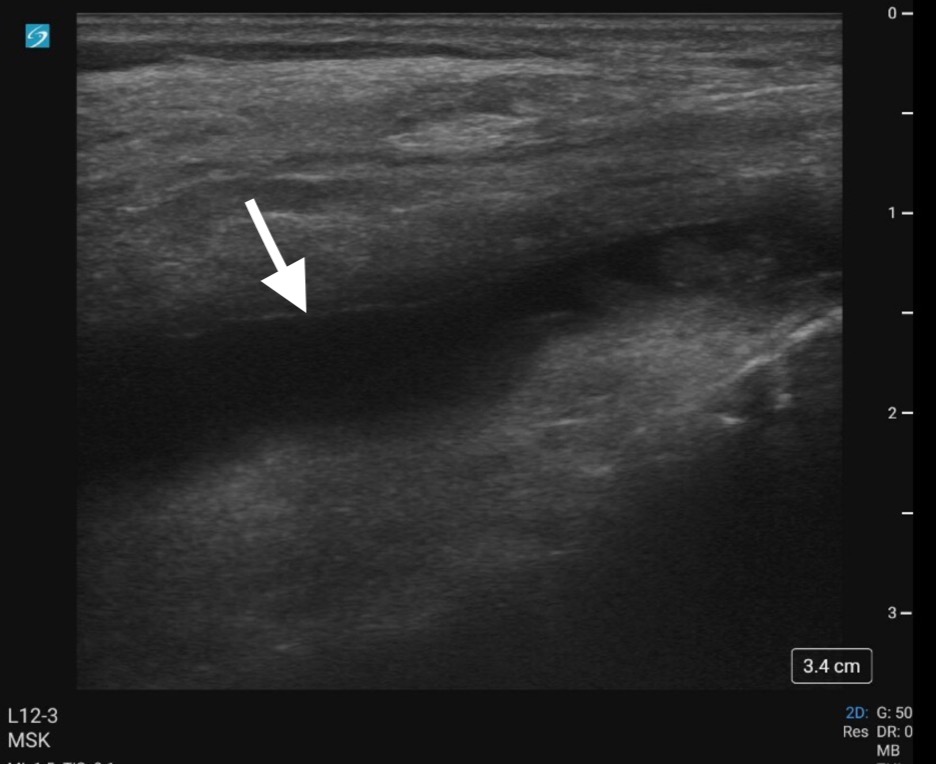
Case Presentation: A 64-year-old woman with a history of sickle cell disease (SCD) from hemoglobin-SS, prior avascular necrosis (AVN) of bilateral hips and humeral heads and prior stroke on chronic exchange transfusions, was brought in by her family for acute confusion and possible increased right-sided weakness. She also reported lower extremity (LE) pain. Neurology consulted and CT/CTA of head and neck showed no acute findings. She received an exchange transfusion at time of admission. On hospital day (HD) 1, she developed acute hypercarbic respiratory failure, attributed to opiate medications, treated with non-invasive positive pressure in intensive care. Her respiratory failure and mental status improved, and she transferred back to floor status HD3. The patient subsequently complained of continued severe pain in LEs, especially bilateral knees and ankles. She was treated with a multi-modal approach for vaso-occlusive pain, including scheduled and as needed oxycodone, as needed hydromorphone, lidocaine patches and pregabalin. Pain remained uncontrolled and she was changed to hydromorphone via patient controlled analgesia. Pain improved though still limited her ambulation. On HD13, she was noted to have bilateral knee swelling consistent with effusions. She reported having been clinically diagnosed with gout in the past due to metatarsal-phalangeal joint swelling though no joint aspiration was done at that time. She underwent ultrasound guided arthrocentesis of her R knee (Figure 1). Joint fluid analysis (Table 1) was positive for monosodium urate crystals.The patient was treated for acute gout, initially with prednisone, then a course of anakinra with initiation of allopurinol and colchicine. Her joint pain significantly improved, and she was discharged home with home health.
Discussion: Hospitalist practioners should be familiar with osteo-articular manifestations of SCD. These include the most common complications, vaso-occlusion and AVN, along with rarer but well described issues such as osteomyelitis.1 Crystalline-arthropathies, particularly gout, have a reported though less well-known association with SCD. While hyperuricemia, present in our patient, is well-described in patients with SCD due to chronic high turnover of red blood cells,2 there have been relatively few case reports of gout in this population.3, 4 However a recent case-control study conducted in Nigeria reported significantly higher incidence of gout in patients with SCD compared with age and gender-matched controls, suggesting that gout may be under-diagnosed in this population.5As our case illustrates, gout can be challenging to diagnose in patients with SCD. For our patient, her initial altered mental status, poorly documented prior gout diagnosis, and prior diagnoses of AVN likely contributed to the delayed gout identification. In a recent case series comparing patients with SCD with versus without gout, hgb SS, higher uric acid level, lower hemoglobin and poor renal function (all present in our case) were more likely among those with gout.6 In addition, large knee effusions, as in our patient, are atypical with vaso-occlusion and should raise suspicion for other processes.
Conclusions: In conclusion, hospitalists should maintain an index of suspicion for gout in patients with SCD and joint complaints. Presence of joint effusion, high uric acid level, and poor renal function should further raise clinical suspicion.
.png)