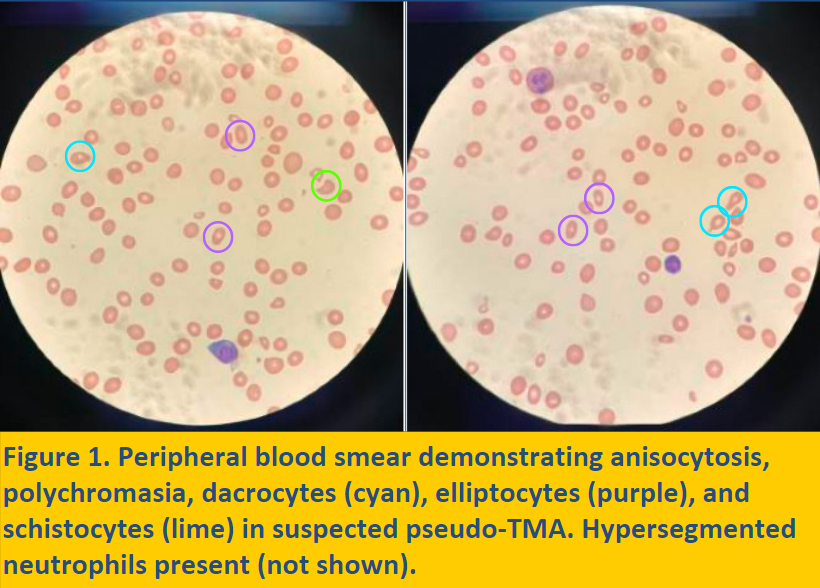
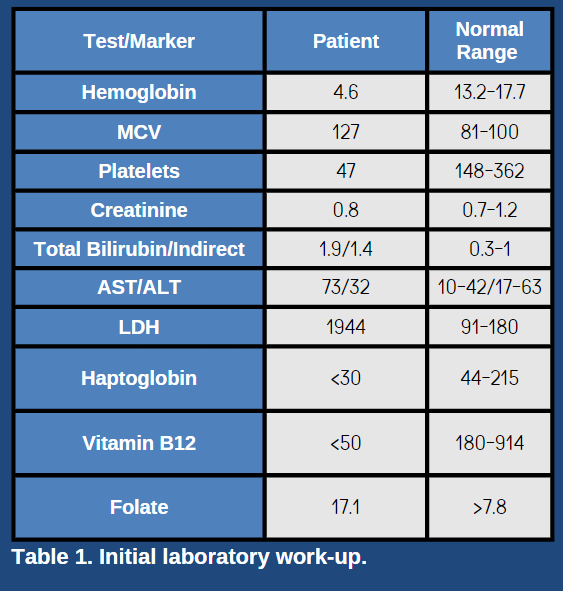
Case Presentation: This is the case of a 39-year-old male with a past medical history of vitiligo presenting for anemia found on outpatient labs. He has a history of anemia on labs 5 years ago that was never evaluated. For the past week, he reported fatigue and dyspnea on exertion. He reported episodes of significant epistaxis for the past two days and passing blood clots. He has also recently noticed yellowing of his eyes and skin. He reports a family history of anemia in several of his sisters. He has worked as a painter for the last 15 years. He reports drinking about 4-6 beers daily, but he abruptly stopped drinking one week ago due to concerns his drinking may be contributing to his anemia. On admission, his initial complete blood count was notable for a Hgb of 4.7, MCV 127, and platelet count of 43.His initial comprehensive metabolic panel was notable for an AST of 63 and a total bilirubin of 2 with predominant unconjugated bilirubin at 1.4, indicating mild liver injury and indirect hyperbilirubinemia suggestive of hemolysis. Urinalysis was within normal limits. Abdominal ultrasound demonstrated evidence of hepatic steatosis. LDH was elevated to 1944 and haptoglobin was undetectable, indicating hemolysis. HIV and hepatitis serologies were negative. Reticulocyte production index (RPI) was 0.38, indicating an inappropriately hypoproliferative bone marrow. Direct antibody testing (was negative. Peripheral blood smear demonstrated hypersegmented neutrophils, decreased red blood cells and platelets, anisocytosis, frequent dacrocytes, and rare schistocytes. His vitamin B12 levels were < 50, indicating severe Vitamin B12 deficiency. Finally, screening for parietal cell and intrinsic factor antibodies was positive, confirming the diagnosis of Pernicious Anemia. Given the hemolytic anemia, schistocytes w/ bicytopenia and likely instigator being a low b12, a diagnosis of Pseudo-Thrombotic Microangiopathy (Pseudo-TMA) was made. While admitted, he received 4 units of pRBCs with subsequent improvement in his symptoms. Prior to discharge, he was started on B12 supplementation and scheduled for outpatient followup.
Discussion: Vitamin B12 deficiency is a common nutritional vitamin deficiency with several etiologies and potential consequences. While Vitamin B12 deficiency can be commonly seen in patients with significant alcohol use, Vitamin B12 deficiency may also arise from etiologies such as Pernicious Anemia, a relatively rare cause of Vitamin B12 deficiency. Patients with a history of autoimmune disease may be at higher risk for developing other autoimmune diseases, such as Pernicious Anemia. Vitamin B12 deficiency can lead to features similar in presentation to TMA, including hemolytic anemia and thrombocytopenia. This syndrome is termed Pseudo-TMA.
Conclusions: Thorough history and workup is critical for assessing for uncommon causes of Vitamin B12 deficiency. A history of autoimmune disease is suggestive of other autoimmune diseases. Vitamin B12 deficiency can lead to features similar in presentation to Thrombotic Microangiopathy (TMA), including hemolytic anemia and thrombocytopenia, as Pseudo-TMA. Early recognition of this syndrome should prompt an assessment for Vitamin B12 deficiency and evaluation for potential causes, such as Pernicious Anemia, given ease of testing. Treatment of this syndrome is simple yet significant, as it can prevent the initiation of unnecessary interventions, such as plasmapheresis, and other complications.