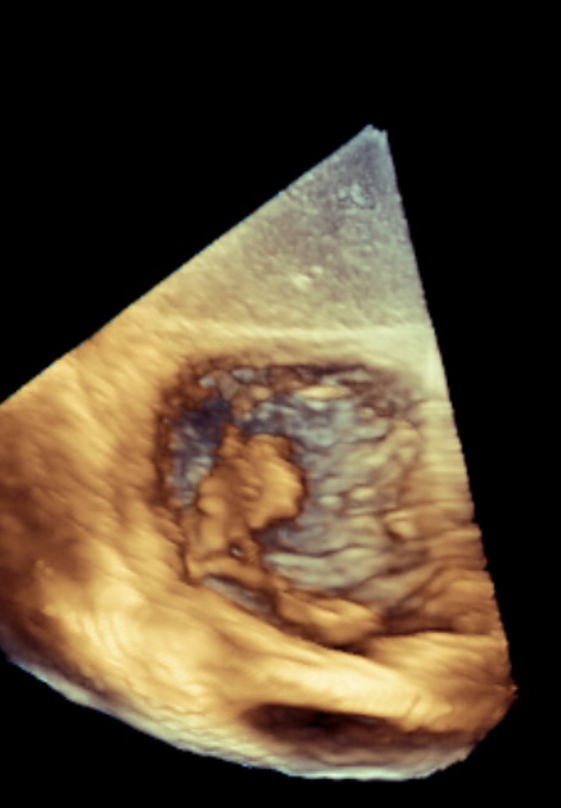
Case Presentation: Managing tricuspid valve infective endocarditis (TVIE) in individuals with intravenous drug use (IVDU) presents significant clinical and logistical barriers. For high-risk patients with limited surgical options, novel percutaneous approaches such as the AlphaVac system, combined with outpatient long-acting antibiotics, offer an emerging alternative to conventional operative management. A 42-year-old man with IVDU and prior lumbar discectomy presented with five days of worsening back pain, fevers, and right lower extremity weakness. Examination revealed lumbar tenderness and motor deficits. Laboratory studies showed leukocytosis (14.8), elevated ESR (69), CRP (24), and D-dimer (3680). MRI demonstrated L5–S1 spondylodiscitis, epidural abscess, and septic sacroiliitis. CT chest revealed bilateral septic emboli, and blood cultures grew MSSA. Transthoracic and transesophageal echocardiography identified a large (2.5 × 0.9 cm) mobile tricuspid vegetation consistent with TVIE. Due to high embolic burden and poor surgical candidacy, percutaneous aspiration with an AlphaVac catheter was performed. Repeat echocardiography after seven days showed near-complete removal of the vegetation, confirming effective percutaneous source control. The patient demonstrated full clinical recovery and was discharged on a 6-week course of long-acting dalbavancin.
Discussion: This case highlights a multidisciplinary, minimally invasive strategy for managing complex right-sided IE in a high-risk IVDU patient. The decision to pursue percutaneous aspiration was guided by the elevated risks associated with open-heart surgery in IVDU including poor wound healing, recurrent infection, and higher perioperative mortality, as well as concerns regarding completion of prolonged IV antibiotic therapy. A catheter-based approach, paired with long-acting outpatient antibiotics, provided effective source control while reducing the need for prolonged hospitalization or central venous access. The patient experienced full clinical and microbiological recovery without recurrence or complications
Conclusions: In carefully selected patients with right-sided infective endocarditis, percutaneous debulking with systems such as AlphaVac may provide effective source control while avoiding the risks of open-heart surgery. This case underscores an evolving treatment paradigm in which coordinated, non-surgical approaches can successfully manage severe IE in populations traditionally considered poor surgical candidates.