Background: Hospitalists frequently encounter patients wishing to leave the hospital before the medical team has recommended discharge (sometimes referred to as “discharges against medical advice” or “patient-directed discharges”). The ethically appropriate response by hospitalists to patients in these scenarios depends on several factors, including the presence of decision-making capacity, the availability of surrogates, the severity of illness, and the type of intervention that may be required by the medical team to implement a hold. Despite the frequency with which these scenarios arise and their ethical complexity, healthcare systems often a lack a systematic, transparent approach to discharges before medical recommendation.
Purpose: To develop an actionable algorithm for hospitalists faced with patients requesting discharge prior to medical recommendation, with clear steps according to well-defined procedures rooted in sound principles that integrate practical, legal, and ethical considerations.
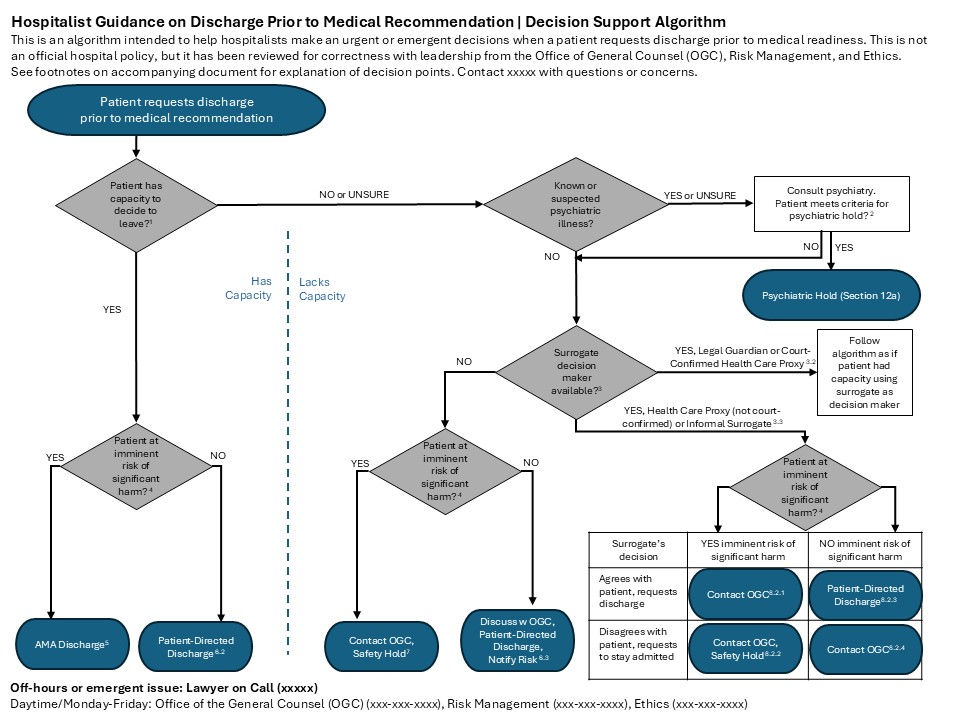
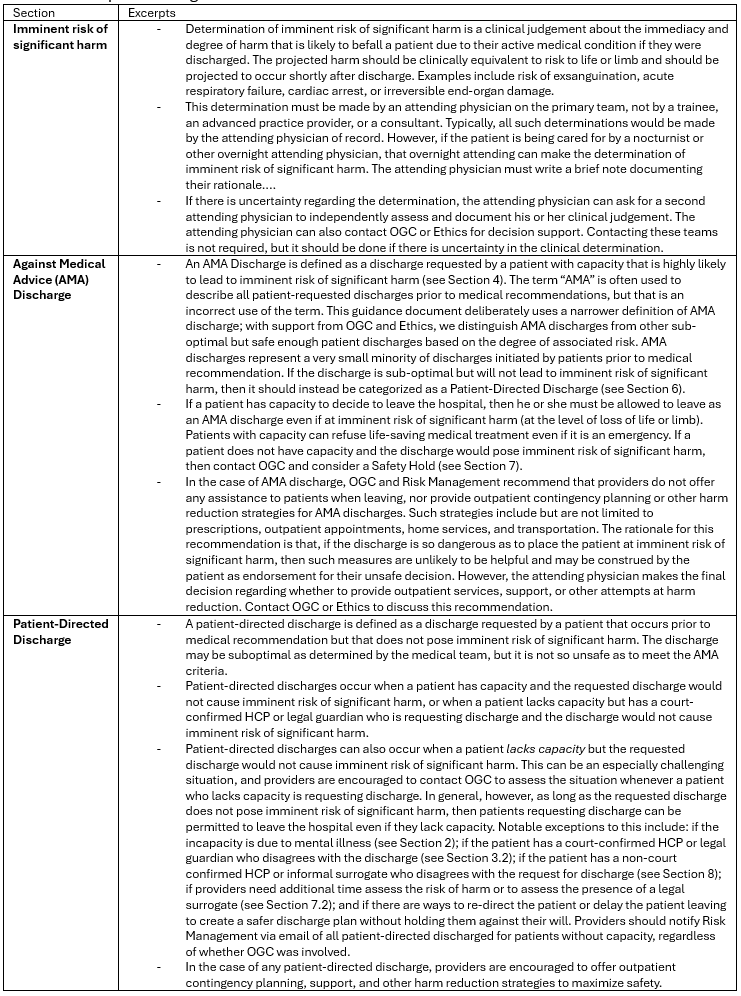
Description: Three hospitalist-leaders identified a need for more clarity about how to handle discharges prior to medical recommendations. We completed literature review of recently published articles, guidelines, and policies at our institution and related institutions to identify best practices. We partnered with the leaders from the hospital Ethics Committee and the Office of General Counsel and, over 9 months, iteratively developed a decision support algorithm with accompanying definitions and rationales based on the best available evidence. The development process included obtaining feedback from stakeholders at Ethics Committee and hospitalist leadership meetings.The algorithm covers key ethical considerations and concepts within state and federal law that arise in decisions about discharge before medical recommendation such as: (1) capacity, including the role of underlying psychiatric illness; (2) surrogate decision-making and how some proxies may have more authority than others; (3) the risk of harm to patients seeking to leave the hospital and how different types of risk may dictate different responses; and (4) the types of interventions that may be permissible depending on the case. The full algorithm is presented in Figure 1 with excerpts from the associated definitions and rationale in Table 1. Several sections were challenging to craft, requiring a consensus that adhered to ethical and legal principles and would be practically useful for the hospitalist managing these situations that typically occur with little warning, conflicting stakeholders, high emotionality, and nuanced ethical and legal risks. Throughout the algorithm, hospitalists are encouraged to contact legal, ethics, and/or risk with questions and for additional support.
Conclusions: Through an interprofessional collaboration, we have developed a systematic approach to managing patients seeking to leave the hospital before medical recommendation. This approach is grounded in core ethical and legal principles for our state and institution while remaining practical for bedside clinicians. Next steps will include revisions based on feedback from hospitalists and working with interprofessional partners in nursing, security, and risk management to operations systems for implementation.