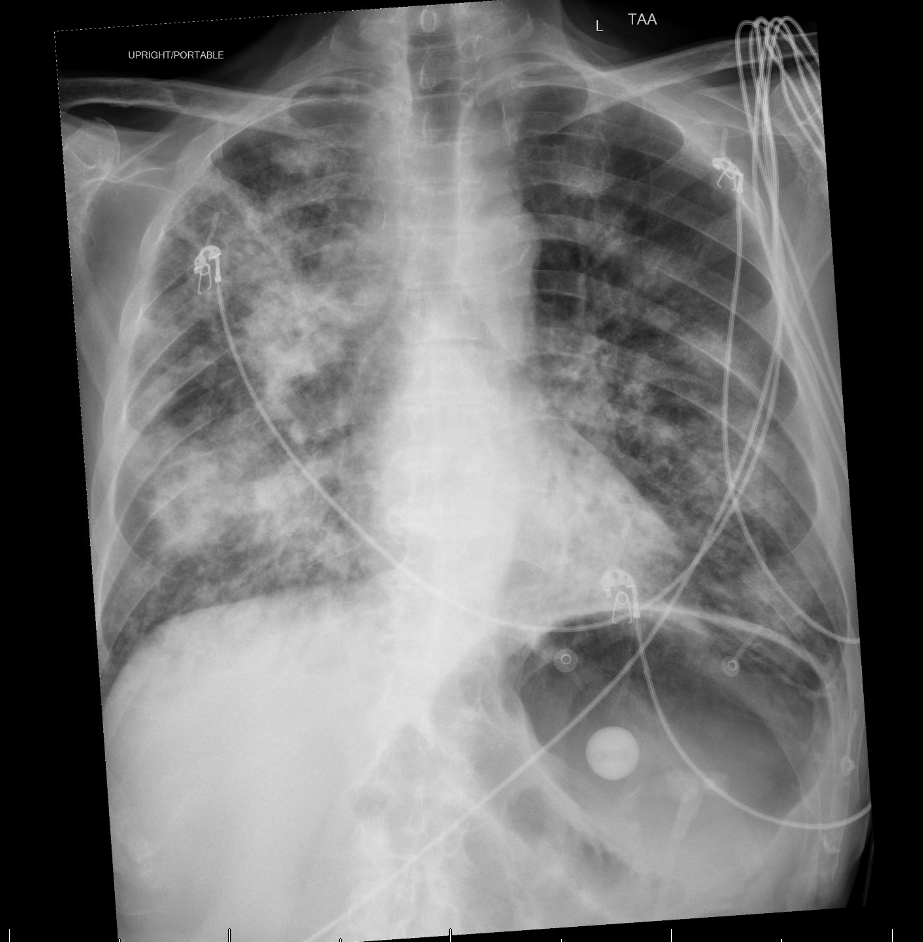
Case Presentation: A 73-year-old male with laryngeal cancer, under treatment at Mayo Clinic and complicated by severe dysphagia and malnutrition requiring PEG tube feeds, was admitted to the ICU with code status of DNR/DNI, with septic shock secondary to multifocal pneumonia. He had two prior admissions for pneumonia in recent months.On admission, empiric therapy with piperacillin–tazobactam and vancomycin was initiated. Blood cultures grew Gram-negative rods, and PCR confirmed carbapenem-resistant K. pneumoniae harboring NDM and KPC carbapenemases, as well as CTX-M (ESBL). Antibiotics were escalated to ceftazidime–avibactam (Avycaz) plus aztreonam.Hemodynamically, the patient required vasopressor support: norepinephrine infusion was titrated from 10 µg/min to 15 µg/min, and vasopressin was added to maintain a MAP ≥65 mmHg. Despite maximal noninvasive ventilation (BiPAP with increased EPAP), his SpO₂ remained in 70–80% range. Palliative care was consulted given his poor baseline health, malnutrition, advanced malignancy and poor prognosis. Despite vasopressor support and noninvasive ventilation, his condition continued to deteriorate. The family ultimately opted for comfort-focused care. The patient died from respiratory and cardiovascular failure secondary to CRE septic shock.
Discussion: Carbapenem-resistant Enterobacteriaceae (CRE) represents an escalating public health threat,recognized by the CDC as requiring urgent and aggressive action. These organisms exhibit resistance to nearly all available antibiotics, often through plasmid-mediated carbapenemase enzymes such as KPC, NDM, and OXA-48, which facilitate rapid horizontal gene transfer. In the U.S., the CDC estimates that approximately 9,000 healthcare-associated CRE infections occur annually, resulting in 600 deaths, with reported mortality rates of up to 50% among critically ill or immunocompromised patients. The burden is particularly high in ICU settings, where bloodstream infections and pneumonia account for the most severe presentations. NDM- and KPC-producing strains are especially challenging due to their extensive resistance profiles and limited treatment options.This case underscores the severity and limited therapeutic options for NDM- and KPC-producing CRE infections, particularly in immunocompromised or medically complex patients. According to the Infectious Diseases Society of America (IDSA) 2023–2024 guidelines, preferred treatments include ceftazidime–avibactam plus aztreonam or cefiderocol monotherapy. NDM enzymes hydrolyze nearly all beta-lactams except aztreonam; however, aztreonam alone is often ineffective due to co-production of serine beta-lactamases (e.g., ESBLs, AmpC, KPC, OXA-48-like). Avibactam inhibits these serine enzymes, and its combination with aztreonam provides synergistic coverage against both NDM and co-produced enzymes. Timely molecular diagnostics and early initiation of appropriate therapy are critical for improving outcomes.
Conclusions: NDM-, KPC-, and CTX-M–producing K. pneumoniae represents highly resistant and life-threatening infections with significant public health implications. This case highlights the importance of early recognition, guideline-directed therapy, and multidisciplinary care. Broader implementation of rapid diagnostics, antimicrobial stewardship, and access to advanced agents such as ceftazidime–avibactam plus aztreonam or cefiderocol is essential for effective management of these formidable infections.
.png)