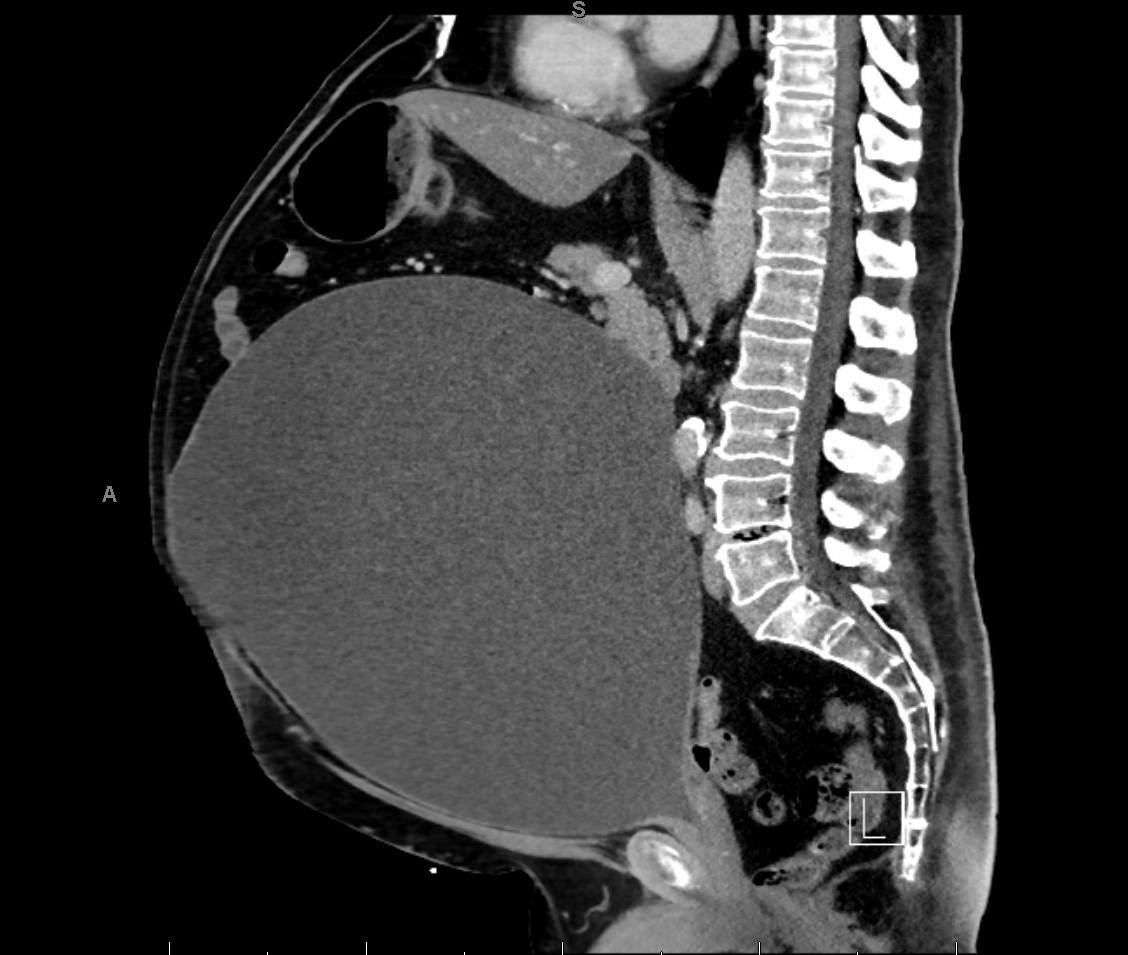
Case Presentation: A 65-year-old male with hypertension, hyperlipidemia, and alcohol use disorder presentedwith sudden severe generalized abdominal pain after a year of intermittent lower abdominaldistention but no urinary symptoms. He denied dysuria, hematuria, frequency, urgency,hesitancy, or recent urologic procedures. Prior outpatient evaluations had suggestedpossible urinary retention, but no definitive diagnosis or treatment had been implemented.In the emergency department, he was mildly tachypneic (RR 23/min) with oxygen saturation>90% on 2 L nasal cannula. Laboratory evaluation revealed preserved renal function(creatinine 1.1 mg/dL, eGFR >60 mL/min), mild transaminitis (AST 122, ALT 131), and risinglactate (2.5 → 3.3 mmol/L). Urinalysis was unremarkable. CT abdomen/pelvis demonstrateda massively distended bladder measuring 31 × 26 × 30 cm. Controlled Foley catheterizationresulted in drainage of 12 liters of urine, confirming chronic massive urinary retention withacute exacerbation. MRI lumbar spine was ordered to assess for potential neurogeniccauses, however it was normal.Management included continued bladder decompression, initiation of tamsulosin, andprophylactic nitrofurantoin. Given the very low likelihood of spontaneous voiding, he wastrained in intermittent self-catheterization with a goal of maintaining post-void residuals < 500mL. He was closely monitored for post-obstructive diuresis and electrolyte abnormalities,and received structured counseling on long-term bladder care.
Discussion: This case illustrates a rare,“silent” form of chronic urinary retention (CUR), with the patientaccumulating an extraordinary 12 liters of urine while remaining largely asymptomatic.Notably, despite extreme bladder distention, his renal function remained preserved.Literature review identifies one case from the United Kingdom reporting drainage of 16liters, the largest known bladder volume. Additionally, an 11-liter case has been reported,situating our patient’s presentation among the largest documented worldwide.These reports underscore the diagnostic challenge posed by asymptomatic or minimallysymptomatic CUR. Untreated massive retention can lead to acute kidney injury, metabolicderangements, infection, and bladder dysfunction. Early imaging, timely decompression, andstructured follow-up including intermittent catheterization and medication optimization areessential to prevent complications and ensure long-term bladder preservation. Hospitalistsplay a central role in recognizing atypical presentations and coordinating multidisciplinarycare.
Conclusions: Chronic urinary retention can remain clinically silent even at extreme volumes, presentingsolely as vague abdominal distention. With documented cases reaching up to 16 liters andonly a few reports of bladder volumes exceeding 10 liters early recognition is critical. Promptimaging, controlled decompression, patient education, and long-term bladder managementare essential to prevent irreversible complications and optimize outcomes.
.png)