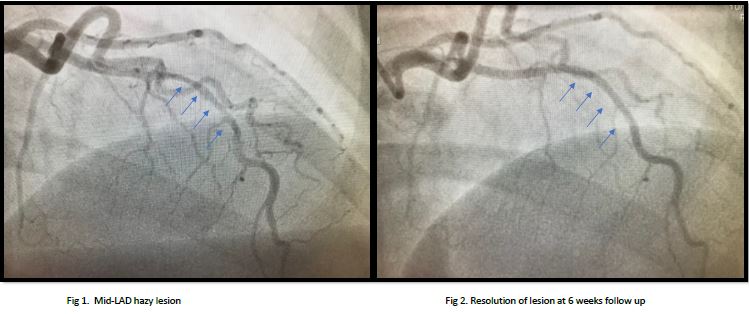
Case Presentation: A 40 year old woman (G4P4A0) with hypertension and hypothyroidism presented with sudden onset, severe, substernal chest pain while lifting heavy garbage bag. She was diagnosed with NSTEMI in the context of typical ischemic chest pain with trending troponins and EKG with T wave inversions in anterior leads. Transthoracic echocardiography revealed apical and anterior regional wall dyskinesia with ejection fraction of 50-55%. Coronary angiography revealed a diffuse and smooth moderate to severe stenosis of left anterior descending artery (LAD). Rest of the coronary vasculature did not show any irregularities, stenosis or obstruction. Patient’s history, presentation and angiographic findings were consistent with type 2 SCAD of LAD. She was managed conservatively with DAPT, beta-blocker, statin and avoidance of physical stress. Work up for associated conditions (renal ultrasound, ANA, ANCA, complement levels) was negative. Repeat coronary angiography 6 weeks later showed complete resolution of previously noted dissection.
Discussion: Spontaneous coronary artery dissection (SCAD) is a non-traumatic and non-iatrogenic injury occurring in the coronary vessel wall. It is caused by either a primary intimal dissection or a primary hematoma in the medial layer. SCAD is an infrequent cause of acute coronary syndrome (ACS), especially in young women presenting with MI. Potential predisposing factors include fibromuscular dysplasia (FMD), postpartum status, multiparity (≥4 births), connective tissue disorders, systemic inflammatory conditions, and hormonal therapy. Up to 20 percent of cases are labeled as idiopathic. It is a diagnostically and therapeutically challenging condition.
Conclusions: SCAD is often underdiagnosed given limitations of conventional angiography. High index of suspicion is needed in young woman presenting with ACS without traditional risk factors for ASCVD. In addition to the diagnostic challenge, the condition poses a major therapeutic dilemma given paucity of literature to guide management. Conservative therapy is favored, except for patients with unstable symptoms, hemodynamic instability, or left main dissection. Patients should be closely followed for long term MACEs including recurrent SCAD. Repeat angiography 6-8 weeks after the index event is recommended to document spontaneous healing. Focused research on the underlying causes, optimal treatment and rehabilitation is needed.