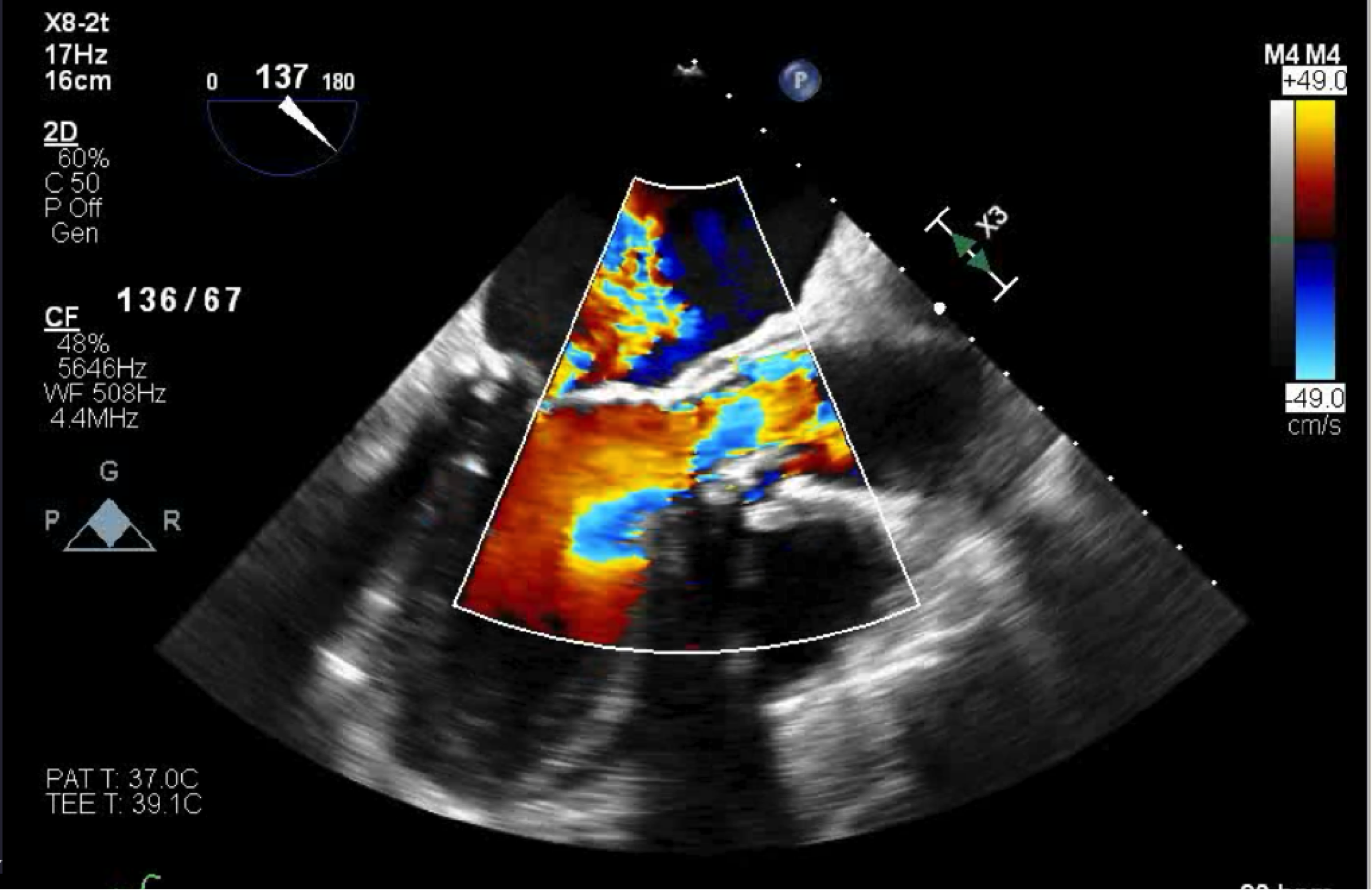
Case Presentation: An 84-year old male with a past medical history of coronary artery bypass graft (3 vessel) 19 years ago, surgical aortic valve replacement (trifecta bioprothesis) 5 years prior, atrial fibrillation on anticoagulation, COPD, Heart failure with preserved ejection fraction, presented to the emergency department complaining of 1 month of shortness of breath and 2 weeks of jaundice. The patient endorsed becoming short of breath after 1 long block. At baseline he had no shortness of breath and participated in bicycle marathons. He also stated other people noticed his skin becoming slightly more yellow. 1 month ago he went to a clinic for the shortness of breath and was prescribed a solumedrol pack and azithromycin. Symptoms did not improve, so the patient presented to the ED for further evaluation. The patient was afebrile with unremarkable vital signs. Physical exam was significant for scleral icterus, fine bilateral bibasilar crackles, early blowing diastolic murmur, JVP 6cm above sternal angle, no S3/S4, no abdominal tenderness, no hepatosplenomegaly, and warm extremities. His laboratory markers were consistent with a hemolytic anemia and concern for intravascular hemolysis, (total bilirubin 3.4 mg/dL, direct bilirubin 1.1 mg/dL, hemoglobin 12 g/DL, hematocrit 38.7%, MCV 96.3 fL, reticulocyte production index 2.035, LDH 625 IU/L, haptoglobin < 7.7 mg/dL), as well as a mild transaminitis (ALT 54 IU/L AST 46 IU/L, alkaline phosphatase 70 IU/L). Direct coombs test was negative, as well as hepatitis panel negative, thin smear showed no blood parasite, acetaminophen and ethanol levels were negative, malaria and babesia immune markers were negative. Right upper quadrant ultrasound showed no evidence of cholelithiasis, cholecystitis, intrahepatic biliary dilation, and common bile duct dilation. Transthoracic echocardiogram showed an EF of 67%. Transesophageal echocardiogram showed severe regurgitation of the aortic bioprosthesis, possible posterior paravalvular leak (PVL), and moderate to severe mitral regurgitation. It was determined that this patient suffered from bioprosthetic valve degeneration resulting in transvalvular aortic regurgitation, possibly PVL, and valvular hemolytic anemia. Transcatheter valve in a valve was done because of the patient’s high Society of Thoracic Surgery operative risk score. During the pre-operative workup, a cardiovascular catheterization revealed the bypass grafts were patent. After the valve-in-valve procedure, aortic insufficiency was not seen on the aortagram.
Discussion: Bioprosthetic aortic valves are becoming more prevalent and we are begnning to see its complications from degeneration. Transcatheter aortic valve replacement for bioprosthetic aortic valve failure has shown favorable survival, improved hemoydynamics, and improved functional and quality of life outcomes.
Conclusions: In patients who have undergone valve replacement, and are presenting with shortness of breath, and bilirubinemia, it is important to keep valvular hemolysis in the differential.