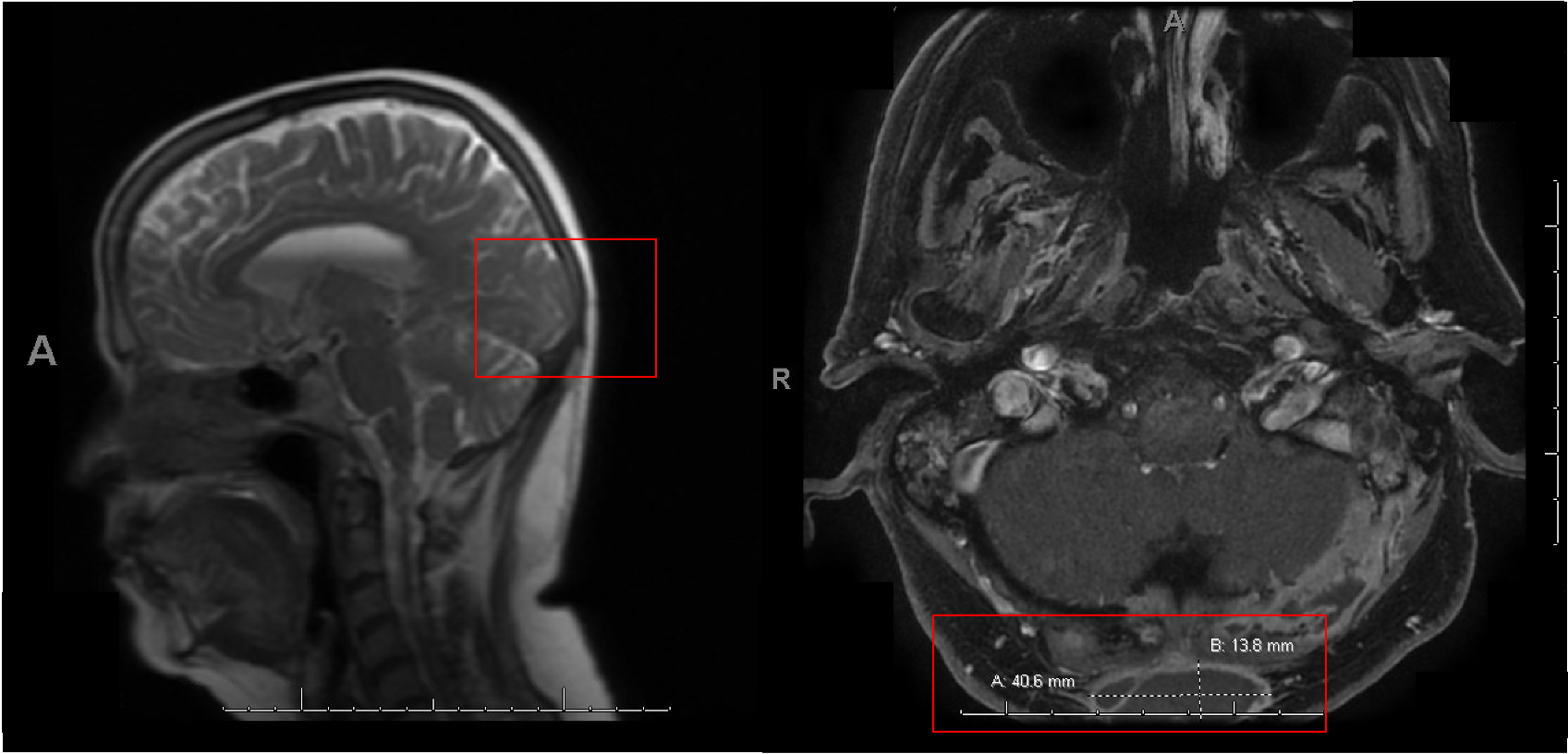
Case Presentation: A 60-year-old woman with no past medical history presented for evaluation of progressive dizziness with associated right-sided hearing loss. On exam, a fluctuant right occipital scalp abscess was noted. CT of the head was suspicious for mastoiditis. She underwent incision and drainage and was subsequently discharged with oral Amoxicillin-clavulanate. Her symptoms persisted for another two months despite repeat incision and drainage of the occipital abscess, two additional courses of varying antibiotics, as well as undergoing myringotomy tube placement. Cultures from her middle-ear fluid and scalp abscess were initially negative. Her right-sided hearing loss and dizziness progressed. MRI showed opacification of the bilateral mastoids concerning for bilateral mastoiditis, confluent enhancement noted within the right middle ear structures suggestive of otitis media, dural enhancement concerning for CNS infection, and osteolysis and destruction of bone and fluid collections spreading to her occipital area concerning for osteomyelitis with overlying abscesses (Figure 1). CT of the chest was also notable for left apical lung cysts. Occipital bone biopsy was performed. Fungal studies performed on prior samples returned positive for budding yeast suspicious for Blastomycosis and her antimicrobial regimen was changed to Amphotericin. Cultures from her bone biopsy, middle ear fluid and occipital abscess fluid all grew Blastomycosis Dermatitidis. Her hearing loss, ear discomfort, CNS and pulmonary imaging findings gradually improved with treatment with Amphotericin which was eventually transitioned to Itraconazole.
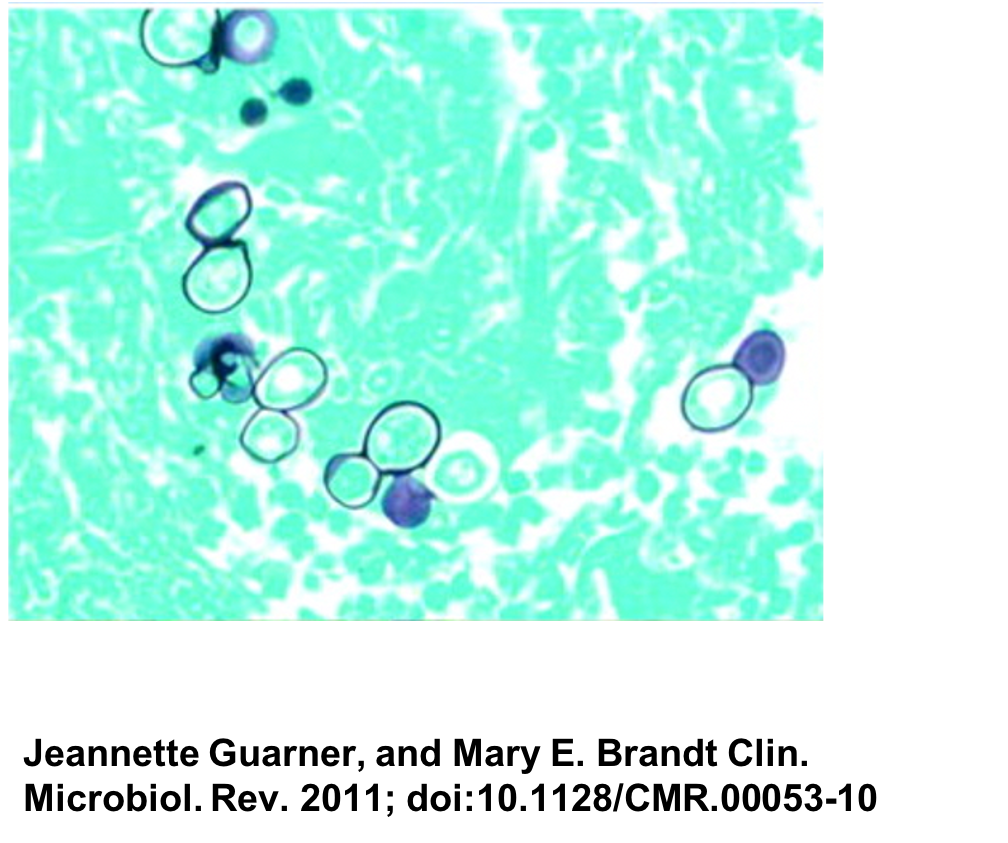
Discussion: Blastomycosis is a fungal infection endemic to the Midwest United States, including the Ohio and Mississippi River Valley regions [1][2]. Infection occurs when inhaled fungal spores transform into yeast forms in tissue [4] (Figure 2). Although infection typically manifests primarily with respiratory pathology disseminated disease may be seen in up to 40% of patients [4]. Disseminated infection may present with cutaneous disease, osteomyelitis, genitourinary or CNS disease [3]. Although cranial osteomyelitis [3] and scalp abscesses are well-documented [6], mastoiditis is less commonly seen [5]. Cultures are often initially negative due to increased time required to grow Blastomycosis in a clinical laboratory and specialized media requirements [4]. Diagnosis can be challenging and delayed diagnosis of Blastomycosis is especially common with extra-pulmonary disease [4]. In fact, one study showed diagnostic delay of over a month in over 40% of patients presenting with Blastomycosis [4]. This patient’s atypical presentation and paucity of pulmonary symptoms made her diagnosis challenging.
Conclusions: Disseminated Blastomycosis may cause culture-negative abscesses and cranial osteomyelitis [4]. A high index of suspicion for fungal infections is warranted for atypical infections in endemic regions to avoid delays in diagnosis.