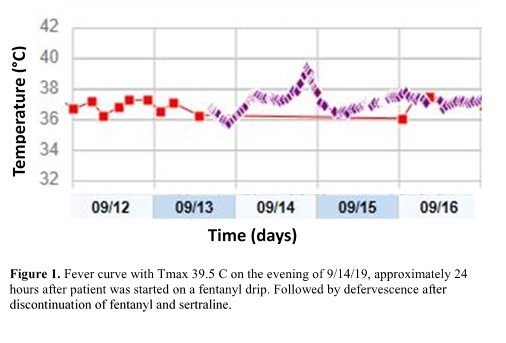
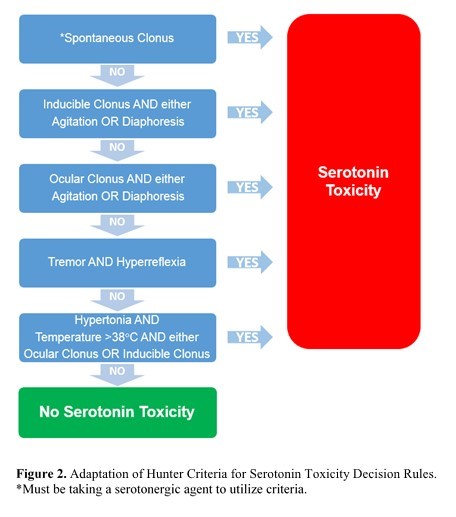
Case Presentation: The patient was a 54yo male with history of alcoholic cirrhosis, CKD, and depression who originally presented to the hospital for a fall, L orbital fracture, and also developed rhabdomyolysis. His hospitalization was complicated by an NSTEMI and he underwent cardiac catheterization with PCI of an anomalous circumflex artery and placement of an intra-aortic balloon pump. He was intubated and sedated with a fentanyl drip, admitted to the cardiac ICU. The next day, the balloon pump was removed, but he required maximum dosing on a fentanyl drip with lorazepam 2mg IV as needed for agitation. He became hypotensive and was started on a low-dose norephinephrine drip. That evening around 2300, he developed spontaneous clonus of his bilateral lower extremities. He was also hyperreflexic. By 0000 he acutely developed a fever to 39.5°C (Figure 1). Routine infectious workup was performed as well as a review of his medication list which included home sertraline 150mg. Based on his symptoms, he met the Hunter Criteria for serotonin syndrome (Figure 2) which was thought to be secondary to initiating fentanyl. The fentanyl drip and sertraline were discontinued, and he received one dose of cyproheptadine 12mg PO and lorazepam 2mg IV as needed for tremor and agitation. He subsequently defervesced that day and had resolution of his spontaneous clonic movements within two days.
Discussion: This case illustrates the importance of recognizing serotonin syndrome quickly as it can cause life-threatening mental status changes, autonomic instability, and neuromuscular hyperactivity. Symptoms typically occur within 24 hours of initiating the offending medication and resolve within 24 hours of discontinuation. Fentanyl is a known serotonergic receptor agonist. The patient’s symptom onset and resolution were consistent with when the fentanyl drip was started and discontinued. It took two days for full symptom resolution, but it was thought that liver and kidney dysfunction may have potentiated serotonergic effects.
Conclusions: Many medications can cause serotonin syndrome, and it often goes unrecognized. Fentanyl is frequently used in critical care and perioperative settings for analgesia and sedation. Prescribers should be aware of its serotonergic activity and monitor for symptoms, especially when patients are on other serotonergic medications, as discontinuation of offending medications is critical for treatment.