Background: High inpatient team censuses are associated with poor patient outcomes, impact trainee education, and contribute to burnout. Since 2019 at the Washington DC VA Medical Center, inpatient medicine team censuses have risen and have been cited as contributing to burnout and decreased educational opportunities. A medical service team expansion was piloted with a goal of reducing the average census of each medicine team by 15% to improve job satisfaction, burnout, and frequency of patient safety events.
Methods: Between February 7 and March 12, 2024, the inpatient medicine service was expanded by creating an additional medicine service team (Team 7) with one resident and one intern, modified from the standard one resident and two intern-based team. The additional team was created by reallocation of house staff from supporting into primary roles and expanded support from interdisciplinary services including social work, case management, and pharmacy. Inpatient medicine team censuses were reviewed retrospectively and monitored in real time prior to and during the 6-week trial. Burnout scores and patient safety perception surveys were completed weekly prior to, during, and post-intervention from trainees and staff. Survey responses were quantified and analyzed to assess the degree of burnout and perception of patient safety. Semi-structured interviews were completed with pilot team participants and evaluated for trends and impressions. Impacts on patient flow were assessed by monitoring interdisciplinary rounding times and discharge smoothing analyses.
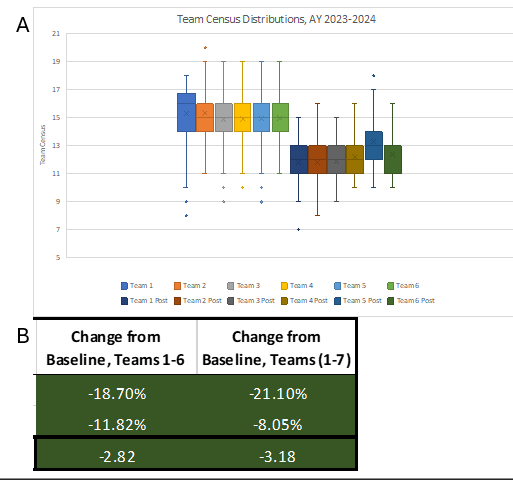
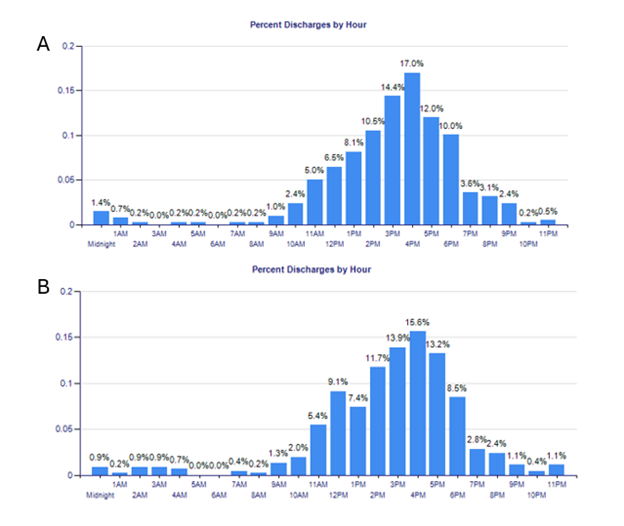
Results: This pilot resulted in an average team census reduction of 18.67% reflecting an average net census decrease of 2.8 patients per team per day (Figure 1), which persisted after adjusting for variations in total hospital census. Discharge frequency before 12 PM improved from 18.26% to 22.54% during the trial; this trend persisted for discharges occurring before 2PM increasing from 37.08% to 41.76% during the pilot study (Figure 2). The proportion of patients with prolonged lengths of stay had a relative decrease of 16.62% during the pilot study, as well. Trainee and staff burnout scores improved from an average of 3.56 to 2.20 reflecting a significant improvement in burnout trends across all levels of training. Perception scores of daily workload jeopardizing patient safety significantly improved with a cumulative reduction in perceived occurrence risk of 56.67% from pre-pilot survey data.
Conclusions: The introduction of a modified inpatient medicine team expansion pilot resulted in improved team censuses, patient flow, and discharge smoothing. The pilot also resulted in significant improvements in subjective staff and trainee job satisfaction and perceived patient safety risks. Further investigations into sustainable implementation and staffing strategies may result in additional improvements in patient flow, patient safety, and professional satisfaction.