Background: A challenge facing many hospital medicine programs is matching provider staffing to daily patient volumes. Staffing models and clinical work schedules are typically built weeks or months in advance, with limited ability to flex up or down in real time based on actual patient volumes. Patient volumes can vary significantly on a daily or weekly basis, and the lack of agility in clinical work schedules can lead to provider dissatisfaction and burnout as well as inefficient use of budgetary resources.
Purpose: The purpose of our project was to develop a tool to aid in daily staffing decisions in order to maintain per-provider volumes within pre-specified ranges. Our objective was to avoid overloading providers during periods of higher volume while also conserving budgetary resources and offering additional time off to providers during periods of lower volume.
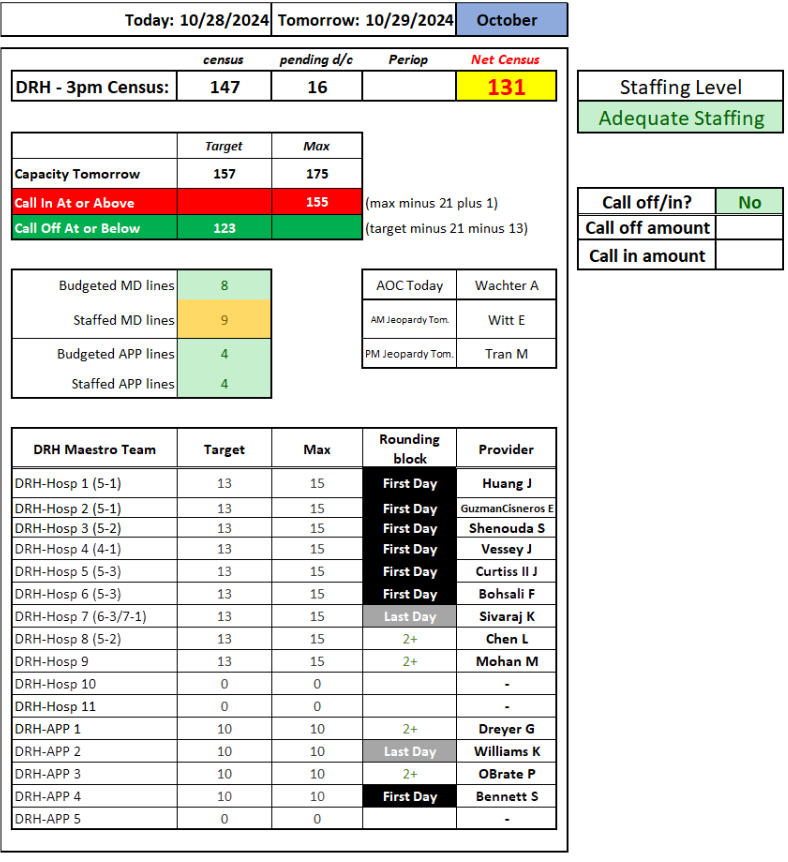
Description: We developed a spreadsheet-based census projection tool that used real-time census data along with historical admission volume data to project per-provider patient census for the following day. On days when projected next-day per-provider census exceeded the predetermined thresholds, our program attempted to add staffing by offering an extra paid shift to providers who were not scheduled to work the following day. On days when projected next-day per-provider census was low enough to reduce staffing without overloading the remaining providers, our program offered a voluntary day off to one or more providers who were scheduled to work. Provider call-offs were done with patient continuity in mind, as only providers who were scheduled to either start or finish a rounding block the following day were eligible to be called off.
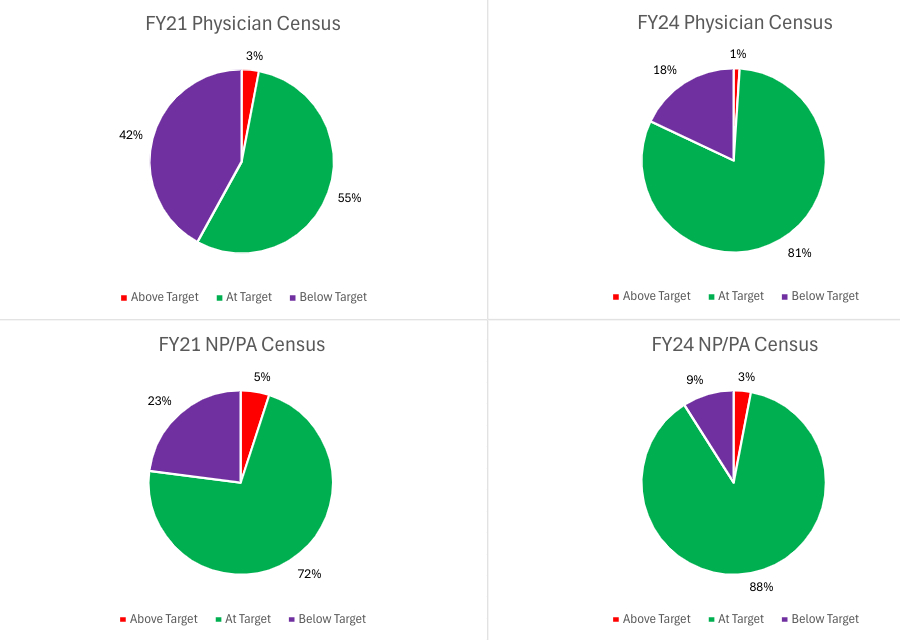
Conclusions: Implementing a census projection tool in conjunction with a system to add or reduce next-day staffing resulted in an increase in the percentage of days when per-provider census fell within pre-specified target ranges. Physician census within target range increased from 55% in FY21, prior to implementation of the census projection tool, to 81% in FY24 after full implementation. NP/PA census within target range increased from 72% to 88% during the same time period. The budgetary impact of implementing a census projection tool and a call-in/call-off system can be estimated by subtracting the savings generated by reducing staffing from the incremental expenditures incurred by adding staffing. In FY24, our program added staffing on 83 occasions and reduced staffing on 39 occasions, at an estimated net cost of $99,600 for the fiscal year. Prior studies have suggested that LOS and overall costs increase with increasing per-provider census, so there may have been additional but unmeasured cost-offsets associated with reducing the frequency of high census days for our providers. Also difficult to quantify is the impact on group wellness that resulted from devoting resources to reducing the variability of provider workload on a day-to-day and week-to-week basis. These topics could be the subject of further inquiry into the impact of improving the agility of hospital medicine clinical work schedules.