Background: At the time of hospitalization, a physician must place an admission status order designating inpatient, outpatient, or observation care. If a patient requires medically necessary hospital care for at least 2 midnights, an inpatient admission order is appropriate. If care is expected to last fewer than 2 midnights or if there is uncertainty about whether a second midnight will be required, observation is appropriate.Condition code 44 (CC44) is a concurrent utilization review (UR) process that applies when a patient admitted as an inpatient is changed to outpatient or observation. This is specific to traditional Medicare beneficiaries and requires UR physician review, an order for outpatient or observation by the treating provider, and delivery of a required Medicare Outpatient Observation Notice to the patient. A separate self-denial process (W2) exists when there is a need to change from inpatient to outpatient status after discharge. The CC44 and W2 processes place specific indicators on the claims submitted to Medicare.The sum of CC44 + W2 represents the total number of instances where inpatient admission status was selected but outpatient or observation would have been more appropriate. This sum divided by all Medicare discharges can be used as a measure of the initial admission status error rate. Since Medicare and commercial payors do not specify which physician should place admission status orders, workflows may vary. There is little prior literature comparing whether selection of admission status is more accurate by ED physicians or by physicians from admitting services.
Purpose: To compare the accuracy of admission status selection by ED physicians versus physicians from admitting services.
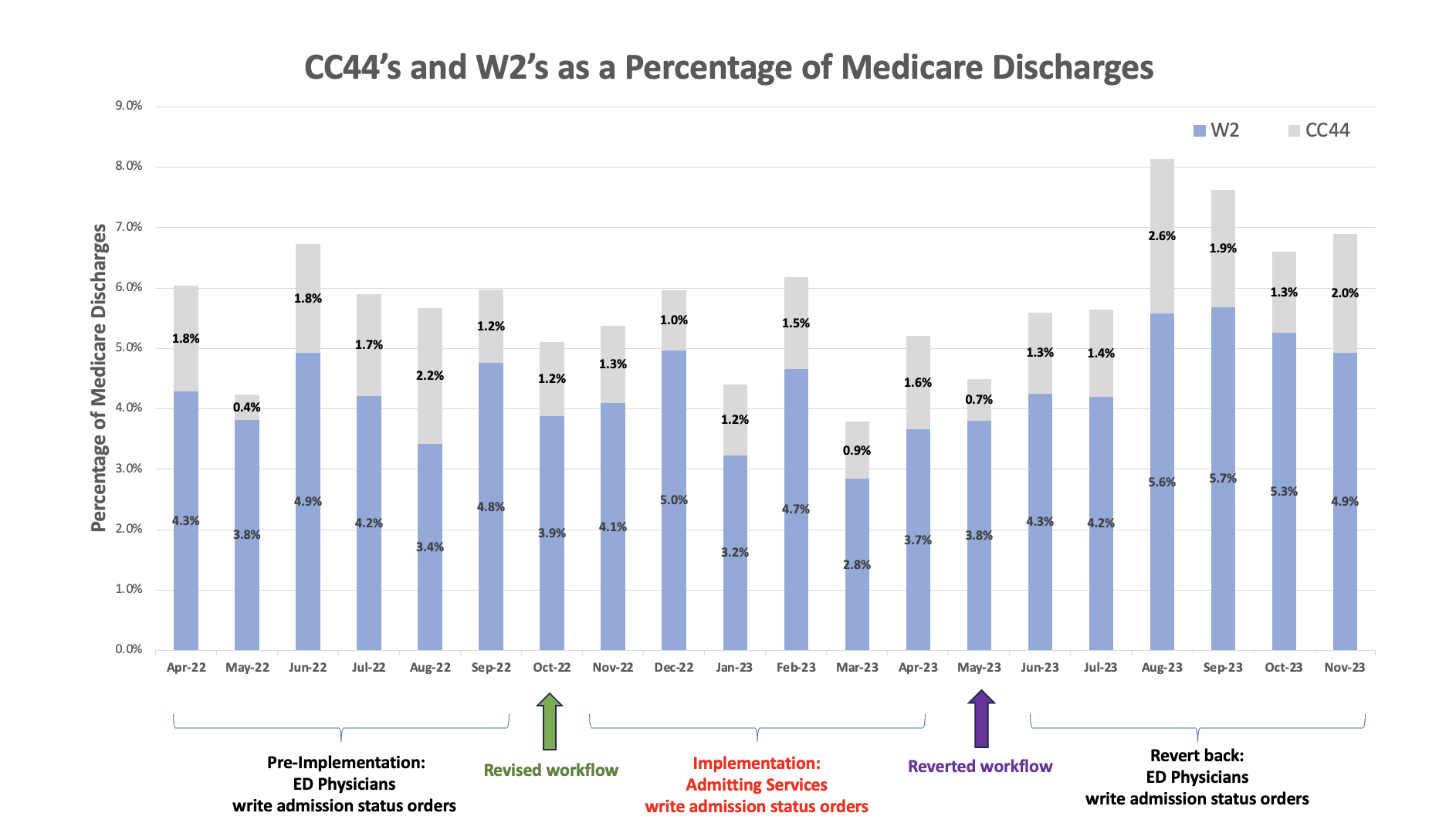
Description: UC San Diego Health (UCSDH) is an 808-bed quaternary care, academic hospital. Prior to Oct 2022, the ED physician entered the hospitalization status order after discussing the case with the admitting provider. On Oct 10, 2022, UCSDH revised EHR workflows to shift responsibility for the hospitalization status order from the ED physician to the admitting physician, postulating that admitting services would be better informed about the plan of care and could make more accurate determinations about admission status. During the 6-month pre-implementation period (Apr to Sep 2022), our average admission status error rate was 5.7%. During the 6-month implementation period (Nov 2022 to Apr 2023), our average error rate was 5.1%. Using an interrupted time series analysis, there was no statistically significant difference in hospitalization status order accuracy with the intervention (level decrease of 0.452%, p=0.65; slope decrease of 0.667%, p=0.52). UCSDH reverted to the prior workflow on May 10, 2023, with ED physicians again entering admission status orders. During the following 6-month period (Jun to Oct 2023), the average error rate was 6.7% (level decrease of 0.028%, p=0.98; slope increase of 1.964%, p=0.07).
Conclusions: There was no statistically significant difference in the accuracy of selection of hospitalization status when orders were placed by ED physicians versus physicians from admitting services at our institution. Since physicians’ familiarity with this topic and associated ordering workflows vary across different institutions, hospitalists can collaborate with their UR team to improve admission status accuracy.