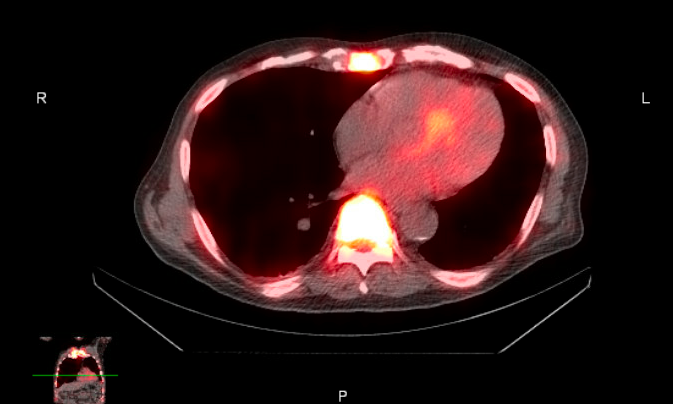
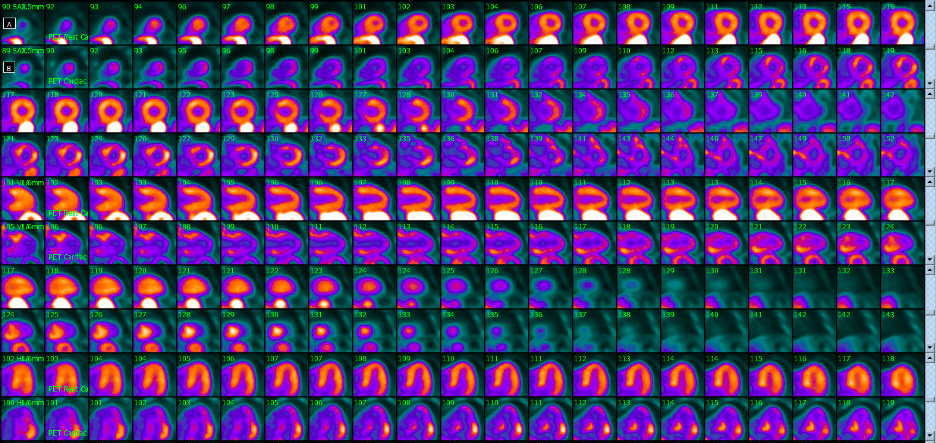
Case Presentation: An 81-year-old man with a history of urothelial carcinoma treated 10 months ago with right radical cystoprostatectomy and nephroureterectomy with ileal conduit followed by seven cycles of adjuvant atezolizumab and tiragolumab, two immune checkpoint inhibitors (ICI), was admitted with malaise, anorexia, and fever for 2 months. His past medical history included left lung adenocarcinoma treated with lobectomy, Mobitz type-II heart block, and stage IV chronic kidney disease. On admission, he appeared fatigued with otherwise normal vital signs and physical examination. Bloodwork revealed leukocytosis (14×109/L), elevated troponin I (0.76 µg/L), and acute kidney injury. He was treated with intravenous fluids and antibiotics for presumptive pneumonia. Transthoracic echocardiogram showed hypokinesis of the basal and mid-infero-septal wall. He was discharged after clinical improvement but readmitted 10 days later with worsening fatigue, rising troponin I (1 µg/L), new hypercalcemia (13 mg/dL), and worsening renal function, as well as new sustained atrial flutter with frequent pauses. Further investigations revealed suppressed PTH, normal PTHrP and 25-OH vitamin D, and elevated 1,25-OH vitamin D (>150 pg/mL). FDG-PET/CT demonstrated diffuse uptake in multiple joints, axial skeleton, and myocardium, with no evidence of cancer recurrence. Cardiac MRI revealed myocardial edema with patchy subepicardial late gadolinium enhancement, indicating a differential diagnosis of sarcoidosis, myocarditis, amyloidosis, or hypertrophic cardiomyopathy. A cardiac sarcoidosis protocol PET/CT suggested active cardiac sarcoidosis, and a PYP SPECT scan additionally suggested amyloidosis. Due to the mixed findings, an endomyocardial biopsy was performed, confirming both active cardiac sarcoidosis and transthyretin amyloid deposits. The patient was treated with steroids resulting in rapid improvement, as well as tafamidis, and he was discharged with outpatient follow-up.
Discussion: ICIs have transformed cancer therapy but are associated with immune-related adverse events (irAEs), including rare cardiac complications such as myocarditis and sarcoidosis. Diagnosing rare cases of ICI-induced cardiac sarcoidosis is challenging, especially when typical pulmonary hilar lymphadenopathy is absent. Following the usual diagnostic algorithm for hypercalcemia helped clinch the diagnosis even in this complex case, as elevated 1,25-OH vitamin D suggested a granulomatous process, particularly in a patient on ICI therapy. Advanced imaging and a multidisciplinary approach were essential for diagnosis and treatment. The presence of previously undiagnosed amyloidosis, likely unrelated to the ICI therapy, further complicated the clinical course and highlights the need for monitoring for acute and chronic cardiac conditions in patients on ICIs.
Conclusions: This case emphasizes the importance of vigilance for rare cardiac irAEs like sarcoidosis in patients receiving ICI therapy, particularly in those with pre-existing cardiac conditions. The co-occurrence of cardiac sarcoidosis and amyloidosis presented diagnostic and therapeutic challenges, requiring a multidisciplinary approach. Further research is needed to develop standardized screening and management protocols for patients with pre-existing cardiac conditions who require ICI therapy.