Background: Early warning scores are used with increasing frequency, but little data exist on the impact of these scores on clinical outcomes. Our health system’s experience with two prior early warning scores was associated with complaints of alarm fatigue and no demonstrable improvement in clinical outcomes. After performing a retrospective validation comparing six early warning scores, we implemented an FDA cleared, EHR-embedded early warning system, eCART (AgileMD, San Francisco, CA), inclusive of (1) a machine learning AI analytic; (2) standard workflows for front-line nurses and rapid response team members; and (3) continuous unit level audit and feedback of performance metrics to drive adoption.
Methods: We performed a pre/post observational evaluation of consecutive adult medical-surgical hospitalizations between January 2023 and September 2025, with a rolling start across 7 hospitals, including 12 months of pre-implementation (baseline) and 12 months of post-implementation (intervention), excluding a 3-month wash-in period at each hospital (Figure). The primary outcome was in-hospital mortality in patients who had an elevated eCART score (i.e. ≥93 out of a maximum 100) for at least one continuous hour during their hospitalization (target population). Secondary outcomes included hospital length of stay (LOS) and cost savings, using our health systems’ estimated figure of $1000 savings per hospital day avoided. Two-sided t-tests, chi squared and Wilcoxon rank sums were used, as appropriate, to compare the baseline and intervention groups, in both the target and non-target populations, and relative risk was calculated for mortality in the target population.
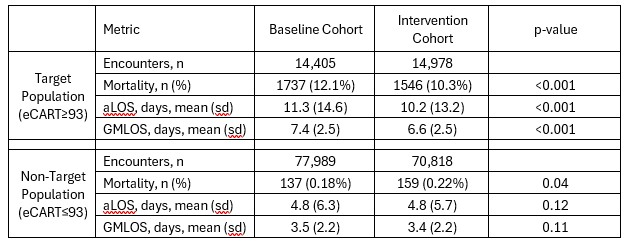
Results: The baseline cohort included 92,394 encounters, of which 14,405 (15.6%) met target population criteria, while the intervention cohort included 85,796 encounters, of which 14,978 (17.5%) met target population criteria. The median age of the target population was 73.1 years and 48.6% were female, compared with 65.3 years and 55.7% female in the non-target cohort, p< 0.001 for both. Baseline and intervention cohort demographics were similar. In the target cohort, mortality decreased from 12.1% at baseline to 10.3% (p< 0.001) during the intervention (Table), resulting in a RR of 0.85 (95%CI 0.80–0.91, p < 0.001). Meanwhile there was a small increase in mortality in the non-target population between the baseline and intervention periods (0.18 vs 0.22%, p=0.04). Average LOS decreased from 11.3 to 10.2 days (p< 0.001) in the target population, without any difference in the non-target population (4.8 vs 4.8 days, p=0.12). Cost savings were estimated at $16,475,800 across the health system (1.1 days x 14,978 encounters x $1000/day) during the 12-month intervention.
Conclusions: eCART identified, in real time, one in six medical-surgical patients with a 60-fold higher baseline mortality and greater than two-fold longer LOS. An EHR embedded workflow intervention targeting this population, utilizing clinical pathways for nurses and RRT members, was associated with a 15% reduction in hospital mortality and 1.1 day LOS reduction which translated into 270 fewer deaths and significant cost savings during the intervention period. These findings highlight the value of pairing real-time risk prediction with structured clinical workflows to achieve measurable improvements in patient outcomes.
.jpg)