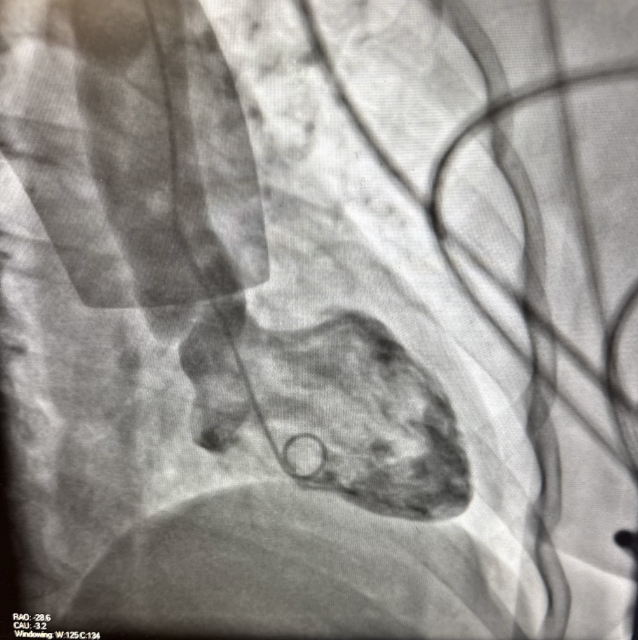
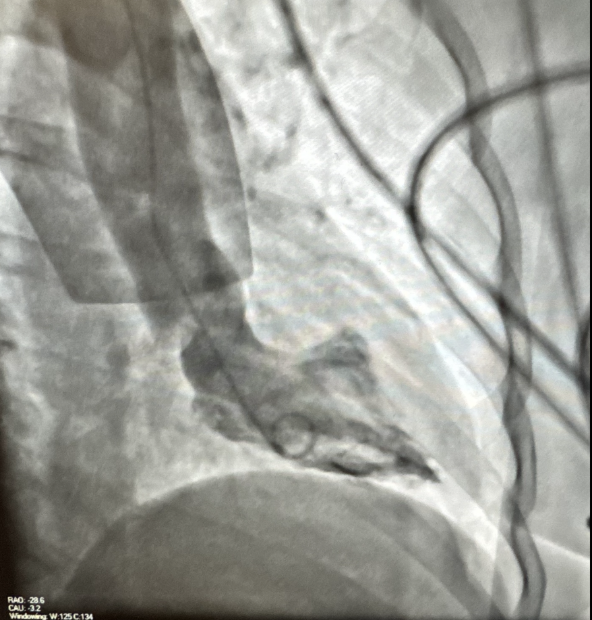
Case Presentation: Takotsubo cardiomyopathy, or stress-induced cardiomyopathy, typically presents with apical ballooning and is often precipitated by emotional or physical stress. We present a rare variant with mid-ventricular hypokinesis in the absence of an identifiable stressor or recent triggering medication.A 66-year-old woman with hypertension, prediabetes, hyperlipidemia, and marginal zone B-cell lymphoma (treated with rituximab, last dose two months prior) presented with nausea, vomiting, and diaphoresis, followed by chest discomfort and shortness of breath. She denied emotional stress, physical exertion, or recent illness. Initial ECG showed sinus bradycardia without ST elevations, but troponins were elevated, peaking above 8000 ng/L. Emergent cardiac catheterization revealed mild coronary artery disease and a preserved ejection fraction of 58%. Left ventriculogram demonstrated mid-ventricular akinesis with hyperdynamic basal and apical segments, consistent with a mid-ventricular variant of takotsubo cardiomyopathy (Figures 1 and 2). Transthoracic echocardiogram confirmed preserved ejection fraction and mild hypokinesis of the mid-anteroseptal wall. The patient remained hemodynamically stable and asymptomatic during hospitalization. She was discharged on aspirin, statin, and beta-blocker therapy with cardiology follow-up.
Discussion: This case highlights a rare mid-ventricular variant of takotsubo cardiomyopathy presenting without an identifiable emotional or physical trigger. The absence of a stressor and the unique distribution of wall motion abnormalities raise important questions about the underlying pathophysiology.Takotsubo cardiomyopathy is thought to result from catecholamine-mediated myocardial stunning, with regional variation in β-adrenergic receptor density determining the affected segment. The classic apical ballooning pattern reflects a higher density of catecholamine receptors and increased sympathetic responsiveness at the apex. This renders it most vulnerable to surges in catecholamines. In contrast, our patient exhibited isolated mid-ventricular involvement with preserved apical and basal function, suggesting an alternative pattern of receptor distribution or signaling.Emerging data propose that receptor heterogeneity, possibly influenced by genetic polymorphisms in β-adrenergic receptor expression or downstream G-protein signaling, may account for the variability in ventricular involvement across takotsubo subtypes. This could explain why some patients demonstrate mid-ventricular or basal variants even in the absence of a clear catecholamine surge. Moreover, her recent exposure to rituximab, while unlikely causative, raises questions about immune modulation and myocardial receptor sensitivity, an area deserving further study.
Conclusions: Recognition of such atypical patterns is critical, as they often mimic acute coronary syndromes yet lack obstructive coronary disease. More importantly, cases like this suggest that takotsubo cardiomyopathy is not a single uniform condition but rather a group of related syndromes caused by catecholamine-mediated myocardial injury. The specific pattern of ventricular involvement may depend on differences in receptor distribution, genetic background, or individual sensitivity of heart muscle to catecholamines. Recognizing these differences can improve understanding of disease mechanisms and guide future efforts in diagnosis, management, and risk assessment.