Background: The interface between two distinct disciplines of medicine with different training regimens and practice cultures can present challenges to effective collaboration. “Few practice-based conceptual frameworks exist to inform interdepartmental QI collaboration in hospital settings, despite a widespread emphasis on QI within hospitals.”.These tensions can be exacerbated by constraints and demands prevalent in healthcare including bed and nursing shortages and an increasing emphasis on efficiency and cost containment. Hospitalists now care for the majority of medical inpatients in sites across the US and are often the first point of contact following evaluation in the Emergency Department. In the context of multiple stressors, the relationship between hospitalists and emergency medicine clinicians can become fraught and conflict prone. We formed an Emergency and Inpatient Medicine Synergy workgroup to identify interdepartmental issues and undertake quality improvement project implementation to improve outcomes.
Purpose: To create effective collaboration between EM and HM to improve patient outcomes and clinician experience.
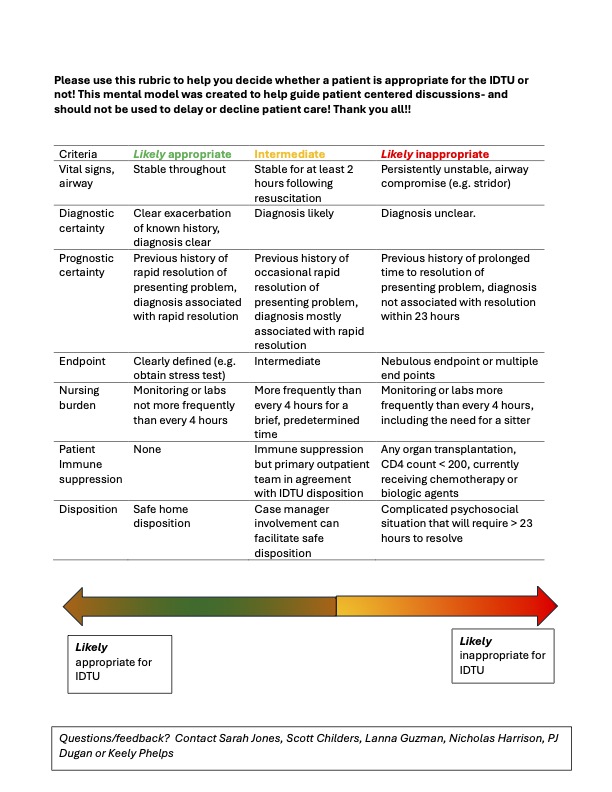
Description: We convened a small group of physicians and advanced practice providers from EM and HM to work collaboratively to identify and address issues that impact patient care with the stated goal of achieving improvements in quality, safety, efficiency, as well as improvement in interdepartmental culture. We codified our purpose through the creation of a mission statement. Project selection criteria were defined, and emphasis was placed on practical issues within the locus of our control. We identified metrics to measure success including the number of projects undertaken, subjective scoring of fulfillment and contribution, project-specific metrics defined by SMART goals, and ratings of collegiality between EM and HM. In the one year since the inception of this group we have jointly 1-Examined the failure rates of patients dispositioned to the 23-hour observation EM-run Intensive Diagnostic and Treatment Unit (IDTU), to identify populations of patients who were appropriate and inappropriate candidates, 2- created guidance to foster a shared mental model of appropriateness for IDTU utilization (Figure 1) 3- created new and accurate data streams to review IDTU utilization 4- improved the electronic communication between EM and HM 5- reviewed care pathways for congestive heart failure 6- created a process for feedback on the appropriateness of patient selection for the IDTU and 7- created of a ‘no- go list’ to help easily clarify which patients are inappropriate for the IDTU. Discussions have fostered group problem solving with a perspective that includes both EM and HM and an interdepartmental review of each individual group’s policies regarding triage workflow as well as disposition decisions.
Conclusions: Our experience with our workgroup to date has been both positive and productive. We anticipate this group will continue to develop future QI projects based in a Plan-Do-Study-Act cycle that will allow for further iterative tests of change in both the IDTU setting as well as in the emergency department and inpatient settings. Engagement in small, iterative changes can help to empower frontline clinicians and improve care and can be effective even in settings that may appear to be in conflict. Focusing on shared goals of patient care, building relationships and communication has the potential to transform care.