Background: Accurate and complete documentation is essential to ensure clarity, compliance, and appropriate reimbursement in hospital medicine. The 2023 Centers for Medicare & Medicaid Services (CMS) Evaluation and Management (E/M) revisions shifted the emphasis toward Medical Decision Making (MDM), requiring providers to clearly articulate the problems addressed, the data reviewed, and the risk of morbidity or mortality. At our institution, fee extractors manually review notes to determine E/M levels. When MDM elements are inconsistently formatted or buried within narrative text, complexity may be overlooked, leading to systematic undercoding despite the provision of appropriate care. This gap highlighted an opportunity to standardize documentation to improve accuracy, completeness, and ease of review.
Purpose: This project aimed to improve billing accuracy, complexity capture, and provider usability through structured documentation tools aligned with the E/M guidelines across hospital medicine providers.
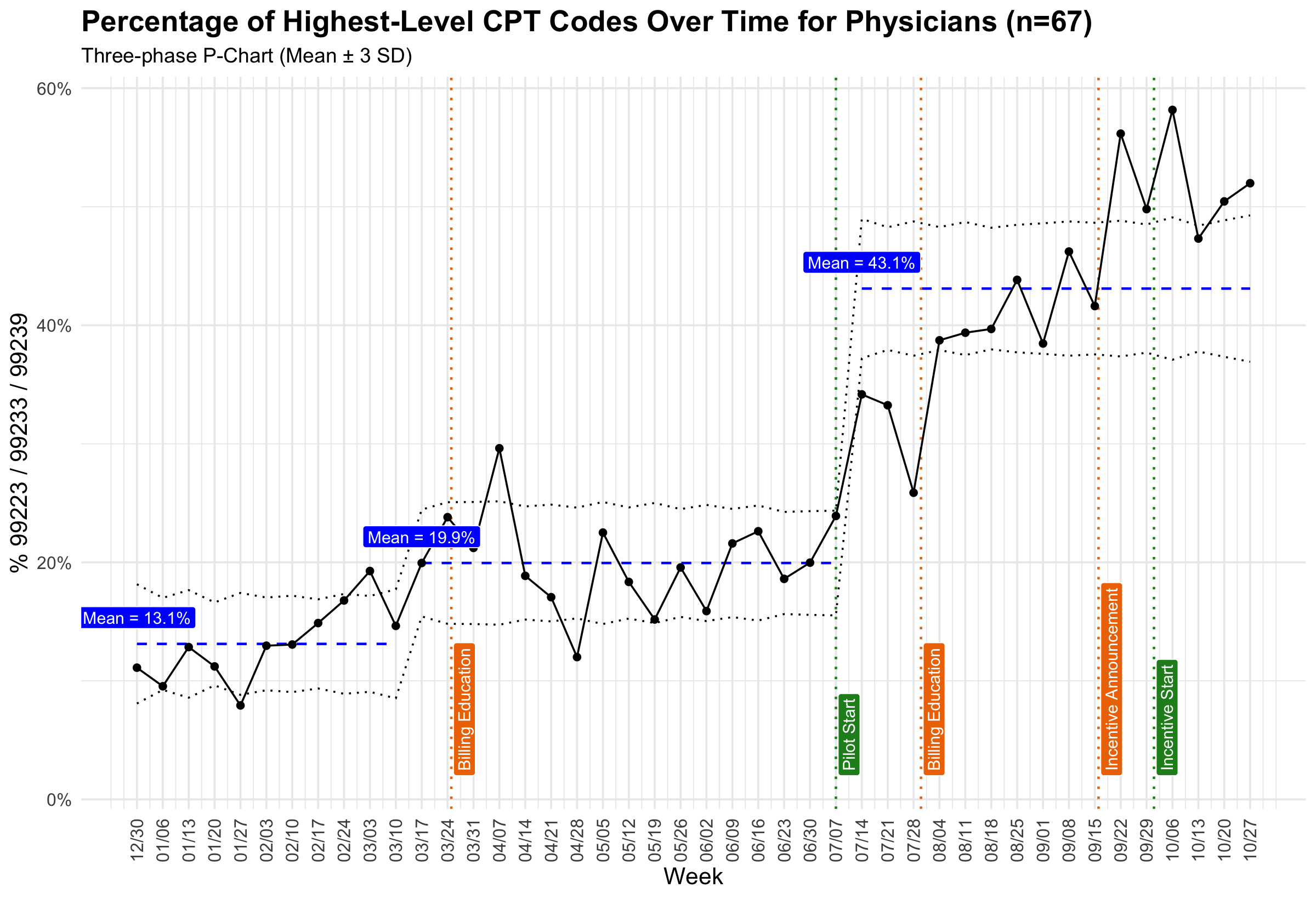
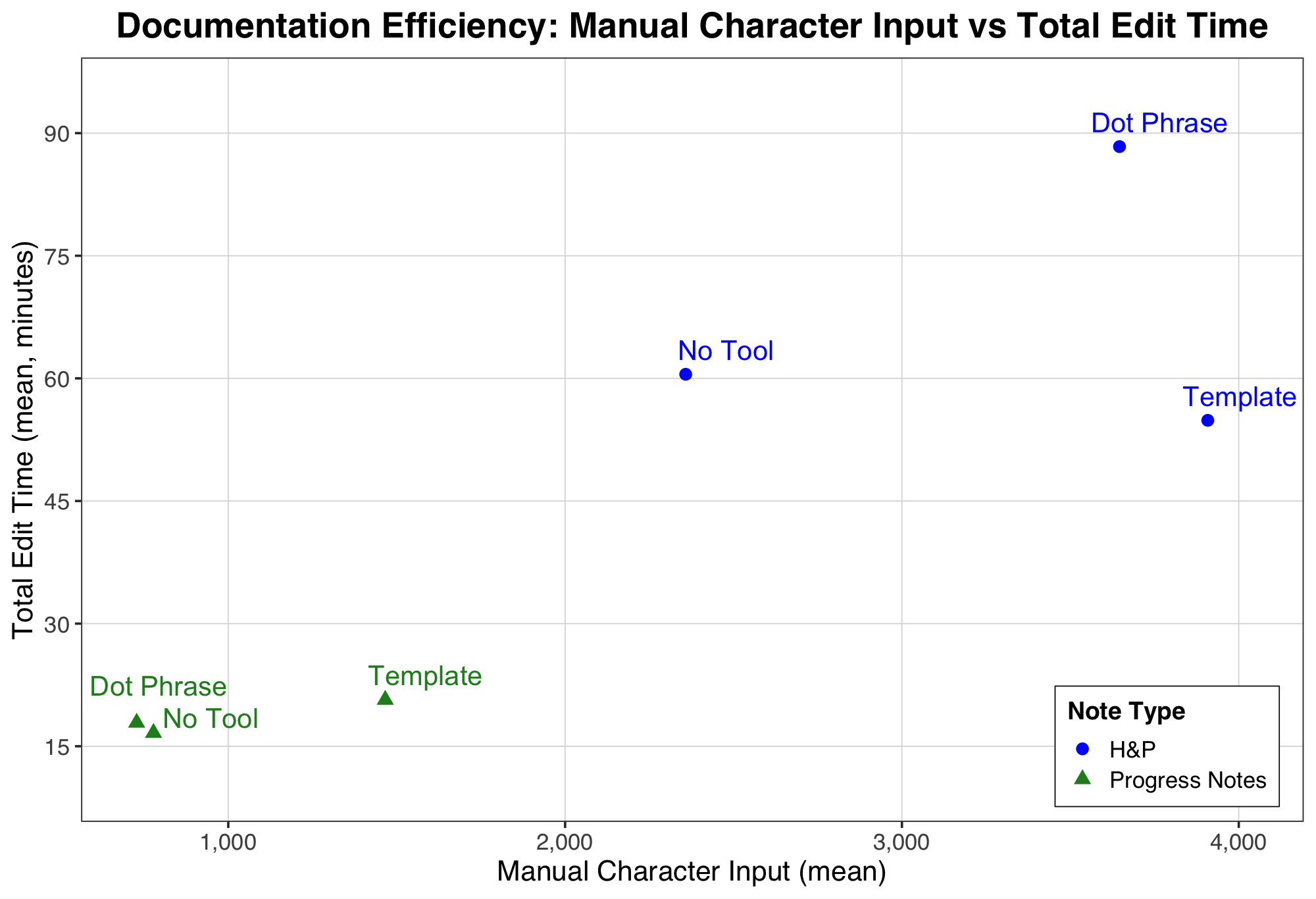
Description: Two documentation tools were developed by informatics, hospital medicine, and billing compliance teams. 1. Standardized note templates for H&Ps and progress notes incorporating MDM lists (complexity, data review, morbidity/mortality risk, time spent) while removing redundant imported data. 2. A modular dot phrase containing the same MDM structure for use within existing templates. Implementation occurred in two stages, first among 23 Advanced Practice Providers (APPs) with gradual expansion to 67 physicians which was tied to a wider individualized incentive-based adoption. Education included tip sheets, videos, and individualized feedback–noting individual feedback was iterative. EHR data were analyzed during the calendar year of 2025. APP tool adoption remained steady over time, averaging 94%. Physician use increased to 95% within one month of the incentive requirement. High-level CPT codes (99223, 99233, 99239) rose from 20% to 46% among APPs and from 17% to 52% among physicians with a strong correlation with tool use (r=0.93, p< 0.001). In our Post-Study System Usability Questionnaire (n = 30), templates were rated more favorably than the dot phrase (2.54 vs. 3.72, p = 0.02), and most respondents reported they would recommend the tool. Additional data collection included the number of characters manually typed by the provider and time to edit notes. This showed that templated HPIs had higher manual input than dot-phrase or non-tool notes, but were completed in less time. In progress notes, templates similarly increased manual input without meaningfully increasing time. These patterns suggest that providers were updating more relevant information without compromising efficiency.
Conclusions: Documentation tools aligned with current billing standards significantly improved billing accuracy and efficiency across hospital medicine services. High adoption was achieved through co-design, targeted education, and incentives. This initiative demonstrates that thoughtful standardization of MDM documentation can enhance clinical, operational, and financial performance while maintaining workflow efficiency. The model offers a scalable framework for enhancing documentation quality and compliance across inpatient settings.