Background: Academic medical centers (AMCs) face growing emergency department (ED) demand, higher ED boarding rates, and reduced capacity for complex community transfers. To “level load” capacity, many AMC’s parter with community hospitals (CH) to transfer lower-acuity patients, yet published transfer rates remain low.
Purpose: To describe the impact of a hospitalist-led intervention to improve throughput and increase appropriate transfers from an AMC to an affiliated CH.
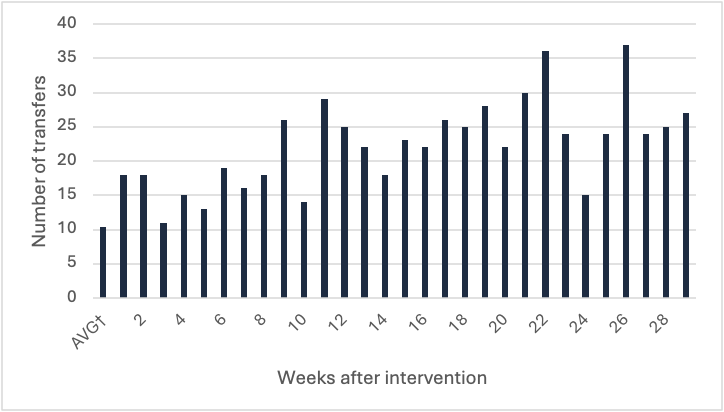
Description: Hospitalists at a large urban AMC led a five-month initiative to expand capacity by increasing transfers to a CH affiliate. They identified three main challenges: limited CH resources, inconsistent eligibility criteria, and inefficient transfer workflows across two systems.1. Community hospital resourcing: Working with CH leadership, hospitalists mapped available consultants, diagnostics, and procedures, then reviewed three weeks of ED admissions to identify high-yield investments. This needs assessment informed system-level changes, including expanded hospitalist admitting capacity, added neurology, gastroenterology, and psychiatry coverage, virtual neurosurgery consultation, and enhanced diagnostic and procedural access (e.g., interventional radiology, stress testing, and CT capacity). Triage protocols were developed for services not available at the CH (e.g. hepatology, advanced endoscopy, step-down care) 2. Eligibility criteria and triage protocols: A triage hospitalist trained in CH capabilities and triage protocols was embedded in the transfer center. Hospitalists developed a mandatory training program and a shared repository of evolving triage protocols. The triage hospitalist documented the rationale for all AMC admissions, and ineligible cases were later reviewed to refine protocols or inform CH service expansion. 3. Triage and transfer workflow redesign: Transfer workflows were streamlined through improved coordination with nursing leadership, bed control, and financial clearance. Hospitalists partnered with ED case management to communicate with patients about the availability of beds at the CH and complete the assent process. In the 52 weeks preceding the intervention, transfers averaged 10.5 patients per week. Post- intervention, this rose to 23.5 per week, peaking at 36 in one week and 125 in one month (Figure 1).
Conclusions: Successful AMC–CH partnerships require aligned resources, explicit eligibility criteria, and standardized workflows. This hospitalist-led initiative doubled transfer volume, demonstrating how hospitalists can operationalize system-level strategies to expand capacity and improve access across hospital networks.