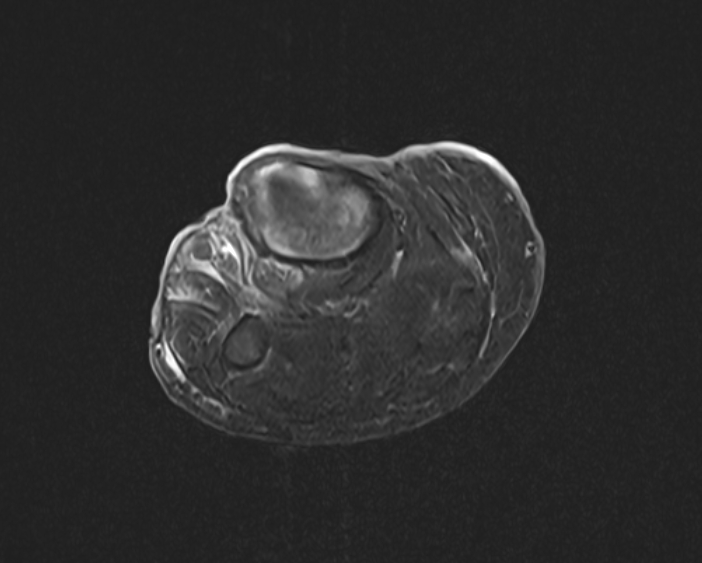
Case Presentation: The patient is a 62-year-old female with a history of a chronic right lower extremity wound and tobacco use disorder who presented to the emergency department for increased discharge from her chronic wound. She states the wound started as a small laceration and has slowly progressed in size for 15 years; she has never sought medical attention in the past. Initial workup was significant for microcytic anemia. An MRI was obtained of the patient’s lower extremity with some enhancement in the affected tibia, indicating possible osteomyelitis. Therefore, vancomycin and piperacillin-tazobactam were ordered out of concern for infection. Due to suspicion for pyoderma gangrenosum, dermatology was consulted, who initiated high dose intravenous methylprednisolone, and gastroenterology performed an upper and lower endoscopy to assess for inflammatory bowel disease. A punch biopsy was performed to confirm the certainty of the diagnosis of pyoderma gangrenosum, however, pathology was consistent with basal cell carcinoma. A repeat punch biopsy from three sites further demonstrated basal cell carcinoma, and bidirectional endoscopy was unremarkable for colon abnormalities. Antibiotics were tapered and steroids were thus discontinued with plans for further dermatology follow up outpatient and eventual initiation of a hedgehog pathway inhibitor.
Discussion: Here we present a case of giant basal cell carcinoma that was initially thought to be pyoderma gangrenosum. Lower extremity ulcers are a common ailment where the vast majority of cases are caused by venous ulcers, arterial ulcers, and diabetic foot ulcers. 10% of ulcers can be categorized as atypical that include other pathophysiologies such as inflammatory, malignancy, metabolic disorders, among others. Pyoderma gangrenosum is a rare inflammatory condition commonly associated with inflammatory bowel disease, hence the investigation of possible IBD in this patient. Recent established diagnostic criteria for PG involve obtaining biopsies to confirm the diagnosis, which was performed in this patient. Giant BCC refers to a subtype that is aggressive in nature and >5 cm in diameter. Giant BCC in the lower limb is rarely characterized in literature and can be misdiagnosed as venous stasis and infectious ulcers; in this case, the ulcer was initially thought to be PG. Once the diagnosis was established, steroids were stopped and antibiotics were tapered. Given the extensive nature of the lesion, the preferred definitive treatment is resection; in our patient’s case, the patient preferred a limb sparing strategy which can consist of Hedgehog pathway inhibitors or radiation therapy to the lower limb. This case reinforces the importance of expanding the differential for lower extremity ulcers to include rarer etiologies such as malignancy, especially those with unusual presentations such as giant BCC.
Conclusions: Degenerative changes can obscure the chronic lesion’s true identity. While our patient’s lesion appeared to be a case of PG, thorough work up and multidisciplinary evaluation revealed a case of giant BCC. This reinforces the importance of including malignancy in the workup of unusual presentations of chronic lower extremity ulcers.
.png)