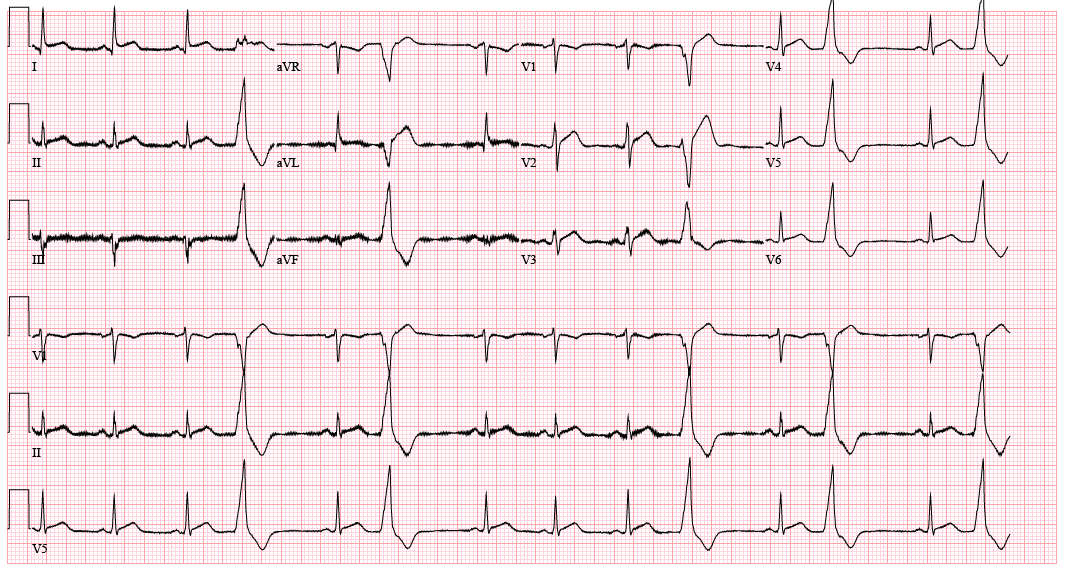
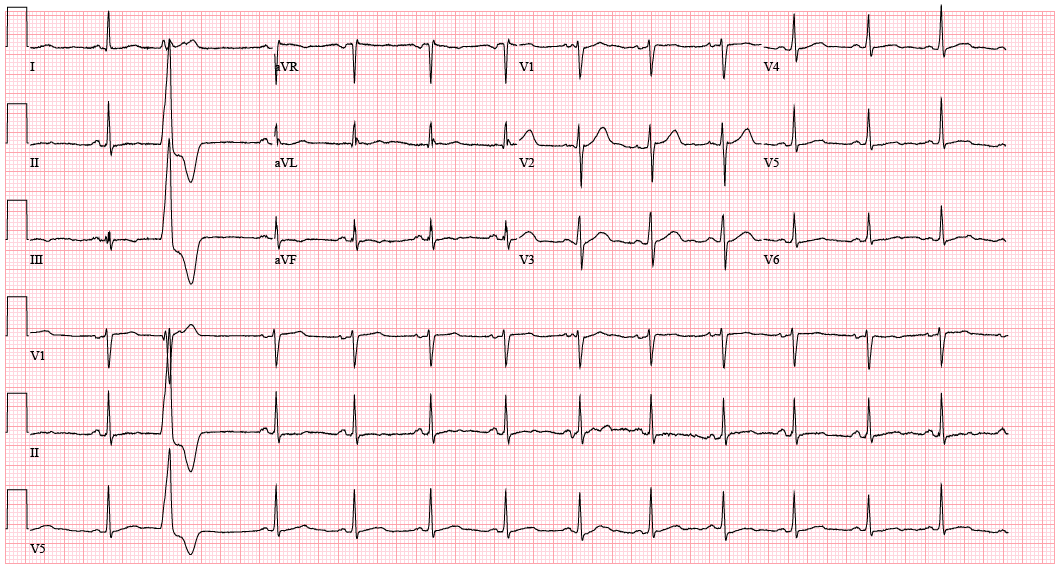
Case Presentation: A 44-year-old man with depression and PTSD presented with five days of progressive nausea and vomiting after ingesting ackee fruit. He attempted home IV fluids, laxatives, enemas, and suppositories. On day 5 post ingestion, he developed worsening epigastric pain. Vitals were normal, but he appeared dehydrated. Labs showed sodium 129 mmol/L, magnesium 4.1 mg/dL, phosphorus 5.3 mg/dL, creatinine 3.27 mg/dL (baseline 1), BUN 97 mg/dL, AST 81 IU/L, ALT 97 IU/L, and metabolic acidosis (pH 7.21, CO2 32 mmHg, bicarbonate 12.8 mmol/L). BNP was 504 pg/mL and high-sensitivity troponin 1 was 1515 ng/L with 1 mm ST elevations in V2, V3, and lead I on EKG (Figure 1). CT abdomen revealed new hepatic steatosis. He received supportive care and was admitted. On hospital day 1 (day 6 post-ingestion), he developed lethargy, bidirectional nystagmus, and asterixis. His head CT was normal. Troponin rose to 4332 ng/L with persistent 1 mm ST elevations in V2, V3, and lead I. Nephrology started sodium bicarbonate. Poison Control confirmed ackee toxicity and recommended supportive care. In the MICU, he was given IV fluids and riboflavin. Troponin peaked at 6524 ng/L, and echo showed a hypokinetic left ventricle with a 30% ejection fraction. Additional labs revealed low TSH and normocytic anemia. By days 7-8 post ingestion, his nausea, neurologic symptoms, renal function, and metabolic acidosis had improved, and he returned to the medical floor. On the following day, catheterization showed normal coronary arteries, suggesting a stress cardiomyopathy over type II myocardial infarction due to demand ischemia. On day 10 post ingestion, he was discharged with metoprolol and empagliflozin. Two weeks later, EKG showed resolved ST changes and no signs of infarct (Figure 2).
Discussion: Ackee (Blighia sapida), a West African fruit, common in Jamaican cuisine, contains hypoglycin A and B toxins (particularly when unripe) that can inhibit fatty acid metabolism and gluconeogenesis, causing mitochondrial dysfunction and a potentially fatal gastrointestinal syndrome known as “Jamaican vomiting sickness”.1 Illness begins within 6 to 48 hours after ingestion with severe nausea, vomiting, and abdominal pain; diarrhea is typically absent.1,2 Severe cases can progress to hypoglycemia and neurologic dysfunction including coma and death within 48 hours.1,3 Rarely, ackee toxicity has been shown to cause acute hepatosteatosis, resembling Reye’s syndrome due to the inhibition of long chain fatty acid oxidation by MCPA.3,4 This patient presented with vomiting without diarrhea, followed by encephalopathy and multiorgan failure, including acute renal failure, thyroid dysfunction, hepatic injury, metabolic acidosis, and stress cardiomyopathy. His abnormal LFTs were concerning for acute hepatosteatosis, possibly via lipid vacuolization of hepatocytes, as in Reye’s syndrome.4
Conclusions: Ackee toxicity can cause multiorgan failure beyond gastrointestinal symptoms. Clinicians should monitor for encephalopathy, AKI, hepatic injury, cardiac involvement, and metabolic derangements.