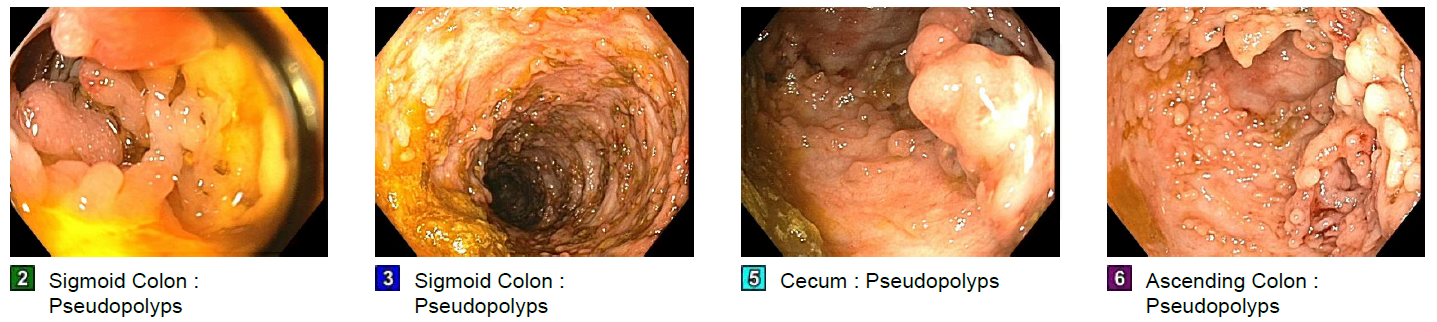
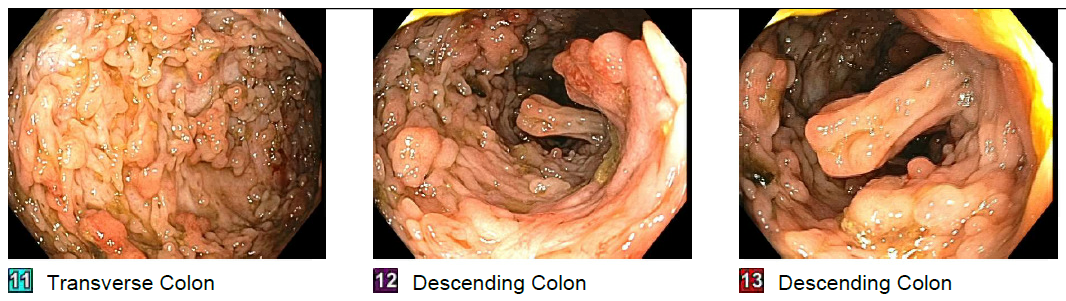
Case Presentation: Inflammatory bowel disease (IBD) is a chronic disease affecting the gastrointestinal (GI) tract consisting of Crohn’s disease (CD) and ulcerative colitis (UC). Patients typically have GI symptoms such as abdominal pain, rectal bleeding, and weight loss. However, the extra-intestinal presentation of IBD is not an uncommon occurrence. Here, we describe a case of a young male patient who presented with severe symptomatic anemia with heart failure, later diagnosed to have CD. Our patient was a 47-year-old Hispanic male with no prior medical history who presented with fatigue, shortness of breath, and lower extremity swelling for 3 weeks. His vitals were stable on admission. Physical examination revealed volume overload and warm extremities. Initial labs were pertinent for severe anemia with hemoglobin 2.3 gm/dl, mean corpuscular volume 63.9 fL and mildly elevated INR 1.3. Iron panel revealed iron deficiency anemia with iron level 16mcg/dl, iron saturation 4%, and ferritin 5.1ng/ml. Further evaluation of the anemia was unrevealing for any overt bleeding, hemolysis, hematuria, or internal bleeding. Echocardiogram revealed low ejection fraction (EF) of 25% with global hypokinesis of the left ventricle. With a presumptive diagnosis of acute systolic heart failure likely from severe anemia, he was promptly treated with transfusion of blood products and diuretics. Further workup with cardiac magnetic resonance imaging (MRI) and cardiac computed tomography angiogram (CTA) was unrevealing. Esophagogastroduodenoscopy (EGD) revealed mild antral gastropathy. However, a colonoscopy revealed diffuse erythema and erosions with pseudo-polyps from the cecum to the descending colon with normal mucosa in the rectum and sigmoid colon. Magnetic resonance enterography (MRE) did not show any fistulas or strictures. Colonic biopsies demonstrated chronic active colitis concerning for CD. His CRP and fecal calprotectin was elevated at 17.7 mg/ml and 1250 respectively. He was started on Prednisone (1mg/kg/day) with plans for initiation of appropriate therapy. Repeat ECHO after correction of anemia showed an improved EF of 35%. His clinical condition improved and he was discharged with a plan for outpatient follow up.
Discussion: It has been noted that about 25% of the IBD symptoms are extra-intestinal involving major organs such as liver, kidney, heart, eyes, muscles, and blood. Among them, more than one-third of the patients present with anemia with a hemoglobin of less than 12g/dl. Anemia in IBD is secondary to a combination of iron-deficiency, chronic inflammation, vitamin deficiencies, metabolic disturbances, and drug therapies. Cardiovascular manifestations usually include myocarditis, pericarditis, VTE and rarely, heart failure. Heart failure is proposed secondary to cardiac re-modelling and myocardial fibrosis secondary to underlying inflammatory state. However, our patient had severe anemia causing high output HF as the first and only presentation of his CD. He did not have any active GI symptoms.In the light of his improved cardiac function with correction of anemia and complete negative workup for other cardiac etiologies, his acute systolic heart failure was attributed to his severe anemia.
Conclusions: It is important to focus on the extra-intestinal manifestation of CD as this could be the only presenting symptom in some patients.