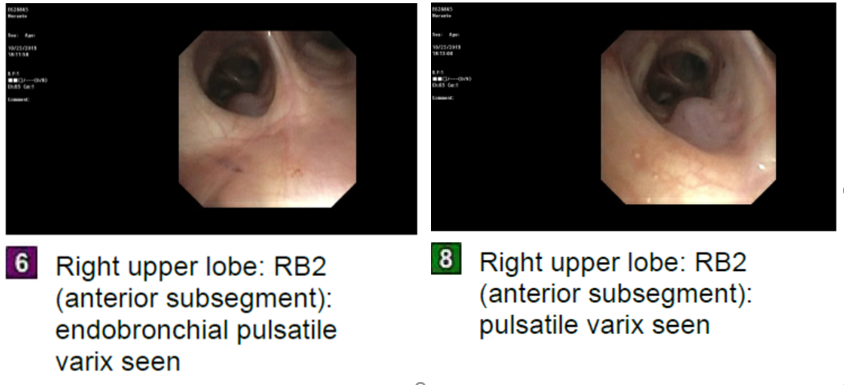
Case Presentation: A 54-year-old never-smoker female with hypothyroidism and rheumatoid arthritis on etanercept presented with intermittent hemoptysis. Three days prior, she reported coughing ~100mL of frank blood and clots (Figure 1) over the course of 24 hours, with smaller volumes over the next two days (~50 mL total). She recounted a similar episode of hemoptysis three years ago without a diagnosis. The patient emigrated to the US over 30 years ago from Ecuador. She reported having multiple negative tuberculin purified protein derivative skin tests. She denied any other symptoms including recent illnesses, fevers, chills, night sweats or a history of epistaxis or gastrointestinal bleeding. There was no family history of nasopharyngeal, pulmonary, or gastrointestinal bleeding. Her heart rate was 102 and her BP was 124/57 on admission. She had anicteric sclera and no mucocutaneous telangiectasias. Cardiovascular exam showed regular rate and rhythm, with no murmurs and no jugular venous distension. Lungs were clear to auscultation bilaterally and abdomen was nontender with no organomegaly. Labs revealed stable hemoglobin at 12.1g/dl, and routine complete metabolic panel with no electrolyte abnormalities or elevated liver function tests. Computed tomography of the chest without contrast revealed focal tree-in-bud nodularity within the RUL and adjacent ground glass densities. Further evaluation with bronchoscopy exhibited multiple endobronchial varices, the largest and most likely culprit of bleeding was pulsatile and in the anterior segment of right upper lobe (labeled RB2 in Figure 2a and 2b). A computed tomography of the chest with and without contrast demonstrated a dilated right pulmonary artery which drained directly into a distal pulmonary vein, suggestive of a pulmonary arteriovenous malformation (PAVM) with feeding artery measuring 2-3mm in diameter. The patient underwent embolization of the right upper, middle and lower lobe branches of the right bronchial artery with resolution of bleeding.
Discussion: PAVMs are an uncommon finding in the general population, with one study showing three PAVMs after 15,000 consecutive autopsies. The most common cause of PAVMs is underlying Hereditary Hemorrhagic Telangiectasia (HHT) (80%-95% of PAVMs), although they can also be associated with cirrhosis, trauma, mitral stenosis, metastatic cancer, and chronic infection (schistosomiasis and actinomycosis). HHT was unlikely in this patient given her negative family history and absence of prior bleeding or telangiectasia. The history and physical were not supportive of the above listed conditions associated with PAVM, indicating an idiopathic etiology. As a diagnosis of exclusion, idiopathic PAVM is a rare finding within the already uncommon diagnosis of PAVM. The patient met criteria for treatment with embolization as she was symptomatic. She also met criteria for treatment based on size alone, as PAVM greater than 2mm in diameter are associated with a 34% prevalence of stroke or brain abscess.
Conclusions: Large volume hemoptysis is a potentially life-threatening acute condition. Although uncommon, PAVMs are an important consideration in the differential diagnosis of hemoptysis, as timely intervention is potentially lifesaving and treatment can prevent associated complications of stroke or brain abscess formation due to paradoxical embolization.