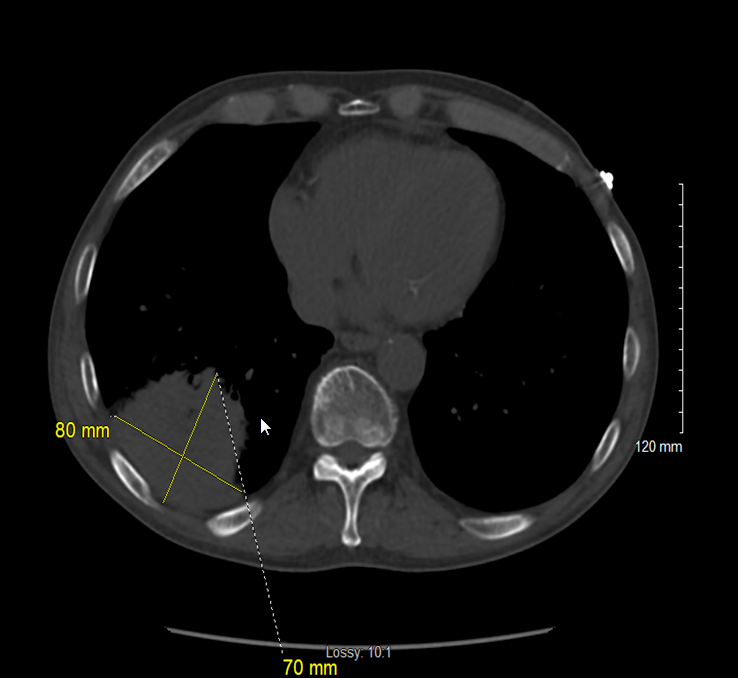
Case Presentation: 71-year-old male with multiple myeloma being treated with dexamethasone, elotuzumab and bortezomib, prior mediastinal plasmacytoma s/p chest radiation therapy and Crohn’s disease was admitted with high-grade fever, chills, productive cough. Labs revealed pancytopenia with neutrophil count of 1.2. Patient was started on broad-spectrum antibiotics for febrile neutropenia. IV Azithromycin was added to the regimen based on positive legionella UA test. CT chest showed 7 x 8 cm large opacity in right lower lobe abutting the pleura concerning for lung mass. Bronchoscopy with BAL showed positive PCR for legionella pneumophila. He showed a good clinical response on IV azithromycin but re-spiked fevers on being transitioned to oral azithromycin. This was attributed to reduced bioavailability of antibiotic secondary to Crohn’s disease. Patient was continued on 5 more days of inpatient IV Azithromycin before switching to oral to complete a 21 day course. He was advised a follow-up chest CT in 4-6 weeks.
Discussion: Legionella pneumonia constitutes 2-8% of CAP cases with high mortality rates of 1 per 10. Patchy unilobar infiltrate is the most common radiological presentation, however in immunocompromised state it may present as pleural based rounded opacity. We present a rare case of a neutropenic host with multiple myeloma currently undergoing chemotherapy who presented with a large dense solid lung mass. It is also important to recognize that while treating pneumonia in hospitalized patients, the presence of crohn’s related diarrhea should be taken into consideration while switching from parenteral to oral antibiotics. Our case started re-spiking fevers when he was started on oral azithromycin. This increased comorbidity and added to his length of stay and hospital cost.
Conclusions: The radiographic findings of legionella pneumophila in an immunocompromised host may vary from nodular infiltrates mimicking invasive fungal infections to solid mass-like lesion. Our report highlights the distinct presentation of legionella in an immunocompromised host. It is also important to recognize that oral azithromycin has a poor bioavailability and thus transition from parenteral to oral should be made cautiously.