Background: Interhospital transfer (IHT) is intended to improve access to specialized therapies, maintain continuity of care, or care concordant with patients’ wishes; however, it is correlated with higher costs, longer length of stay, and greater mortality for many patients, even after illness severity adjustment (1-5). A better understanding of frontline providers’ reasons to accept transfer will help refine appropriate transfer criteria for better management of IHTs.
Methods: We conducted a cross-sectional survey of 11 geographically diverse hospital medicine programs within the Hospital Medicine Reengineering Network (HOMERuN). Surveys were sent weekly x 3 weeks to attending hospitalist physicians involved in the triage of IHT requests, asking respondents how frequently they currently consider and should consider various factors when triaging IHT requests, via 5-point Likert scales (range “Never” to “Almost Always”). Factors included: need for specialty procedural or non-procedural care, bed capacity, continuity of care, covid-related care, patient-family preference, insurance. Optional write-in responses were allowed. The survey also queried respondents’ level of experience and whether they received triage training. Responses were dichotomized into “highly considered” (“almost always”, “more than half the time”) versus “less considered” (“half the time”, less than half the time”, “never”). We used descriptive statistics to report frequency of “highly considered” factors, and conducted z-test of proportions to examine for differences in response by experience level. For write-in responses, 2 independent reviewers conducted qualitative analysis and coded responses into themes within a priori domains, resolving differences through discussion to reach consensus.
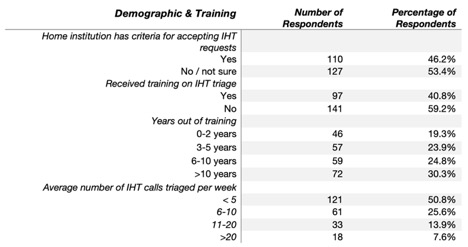
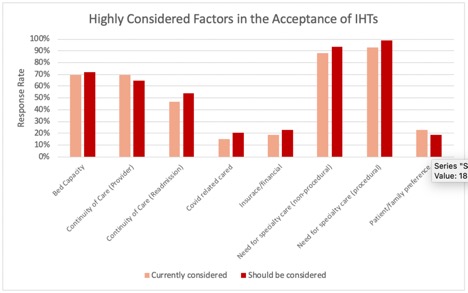
Results: Of the 666 hospitalists surveyed, 238 (36%) responded. Respondents had varied experience and IHT triage training (Table 1). The most frequent reported factors that are both currently and should be considered when triaging IHT patients include: (1) need for specialty procedural care, (2) need for specialty non-procedural care, and (3) bed capacity, with other factors considered less frequently (Figure 1). Respondents with > 6 years’ experience more frequently considered patient/family preference compared to those with 0-5 years’ experience (12.4% vs 4%, p< 0.05). Qualitative analysis in the domain of Criteria for Acceptance identified a theme of consideration of alternatives to transfer if requiring non-procedural care (e.g., tele-consult). In the domain of Threshold for Acceptance, we identified 3 themes: (1) An “accept all” mentality due to a sense of responsibility to the transferring hospital; (2) A low threshold for acceptance due to fear of litigation; and (3) A calibrated threshold of acceptance based on bed availability (e.g., higher threshold for limited bed capacity).
Conclusions: In this national sample of hospitalist physicians responsible for triaging IHT patients, we found that there is general agreement between primary factors that are currently and that should be considered during triage of IHT requests, with greatest weight placed on patients’ need for specialty care. We also identified several themes that impact clinicians’ threshold for acceptance. Collectively, these data help provide an important perspective on hospitalist management and triage of IHT.