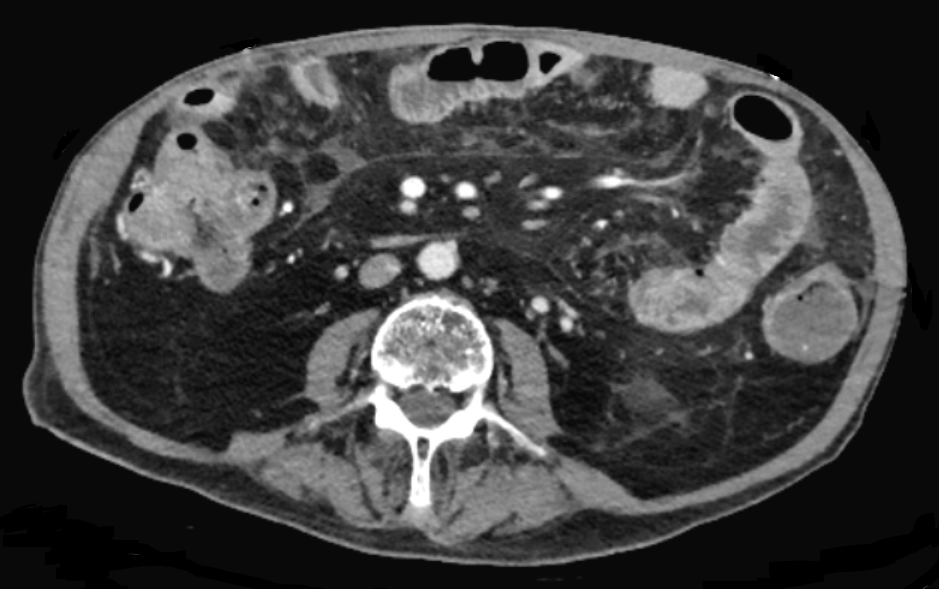
Case Presentation: An 82-year-old man was admitted to our hospital for 3 months of progressive generalized abdominal pain, anorexia, and constipation. He had a medical history of bladder cancer and had undergone radical cystectomy and urostomy via ileal conduit. He had pelvic recurrence of disease 8 months prior to admission and started abdominopelvic radiation (60 Gy in 30 fractions over 6 weeks). His symptoms began 1 week after the final fraction. He had no vomiting, blood in the stool, arthritis, rash, or other symptoms. Medications included high-dose opioids. On examination, vitals were stable. His abdomen was distended, silent to auscultation, and tympanic to percussion. There was severe pain with light palpation and rebound tenderness in all quadrants. Initial labs were unremarkable. Testing for enteric pathogens including C. difficile was negative. CT showed diffuse bowel wall thickening and colonic dilation with associated mesenteric fat stranding, vascular engorgement, and liquefied stool without obstruction. Radiation enterocolitis (REC) was suspected.The patient was treated with empiric antibiotics, reduction in opioid doses, and other supportive care. Bowel function returned with diarrhea, but his abdomen remained peritonitic. Upper endoscopy was performed and push-enteroscopy attempted, but the involved regions of the small bowel could not be reached. Colonoscopy could not be performed due to difficulty with preparation and perceived procedural risk. His subsequent hospital course was complicated by C. albicans fungemia, and the patient died on hospital day 27.
Discussion: Enterocolitis is a common syndrome encountered by general internists and hospitalists. Its etiology is most commonly infectious, but autoimmunity, ischemia, medication toxicity, and infiltration should also be considered depending on clinical context. REC is characterized by cellular injury with leukocytic inflammation and occlusive vasculitis causing disruption of gut mucosa. Severity is dose-dependent and acute gut toxicity begins at cumulative doses of 10-20 Gy. No specific therapies are found to aid resolution, and treatment is supportive. This case offers two additional lessons. First, simultaneous opioid-induced constipation may obscure gastrointestinal diagnoses that typically present with diarrhea. Second, peritonitis can occur from various diffuse intra-abdominal processes that cause sufficient inflammation, and does not always represent surgically treatable disease.
Conclusions: Radiation toxicity is in the differential diagnosis of enterocolitis. Cases can be mild and self-limiting, or severe as demonstrated by this case. The effect of opioids on the gut can alter natural history and contribute to bowel dysfunction.
.png)