Background: Hospitalized patients with COVID-19 who improve clinically but have ongoing oxygen requirements are often discharged with home oxygen. There are important considerations for home monitoring, follow-up and education at the time of discharge for these patients who must manage new equipment at home. This project aimed to describe discharge planning for COVID-19 patients with new home oxygen and to explore patient/caregiver experience of the care transition, with the goal of identifying areas for improvement.
Methods: Patients with COVID-19 at an academic quaternary care center who were discharged from the Medicine service with new home oxygen were identified from social work referrals for home equipment from December 2020-March 2021. Information collected included rates of 30-day readmission, written discharge instruction provided, and follow-up appointments scheduled. Patients or their primary caregivers were invited to participate in a telephone survey which assessed explanation of home oxygen use, delivery, ease of use, and patient awareness of follow-up appointments.
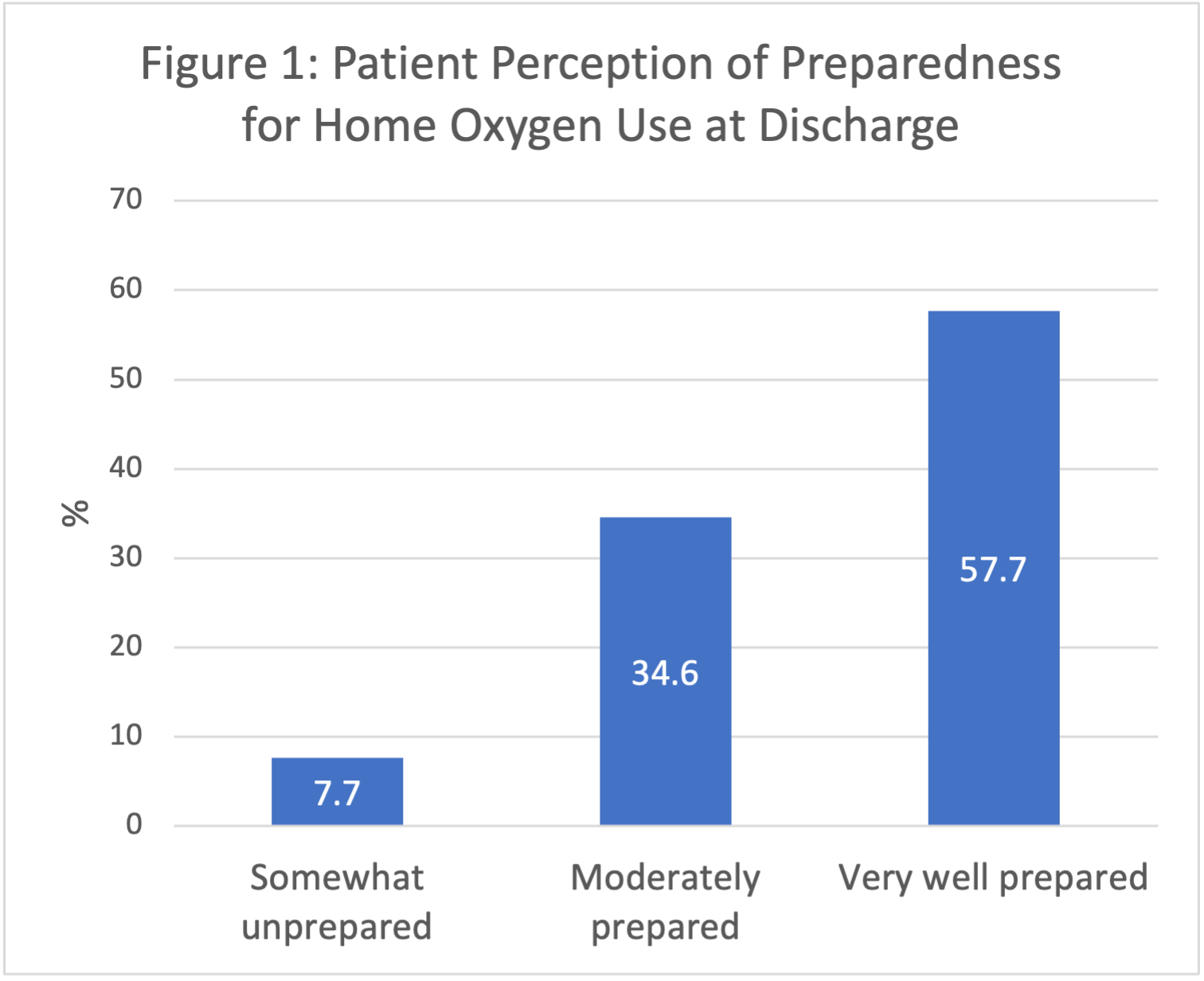
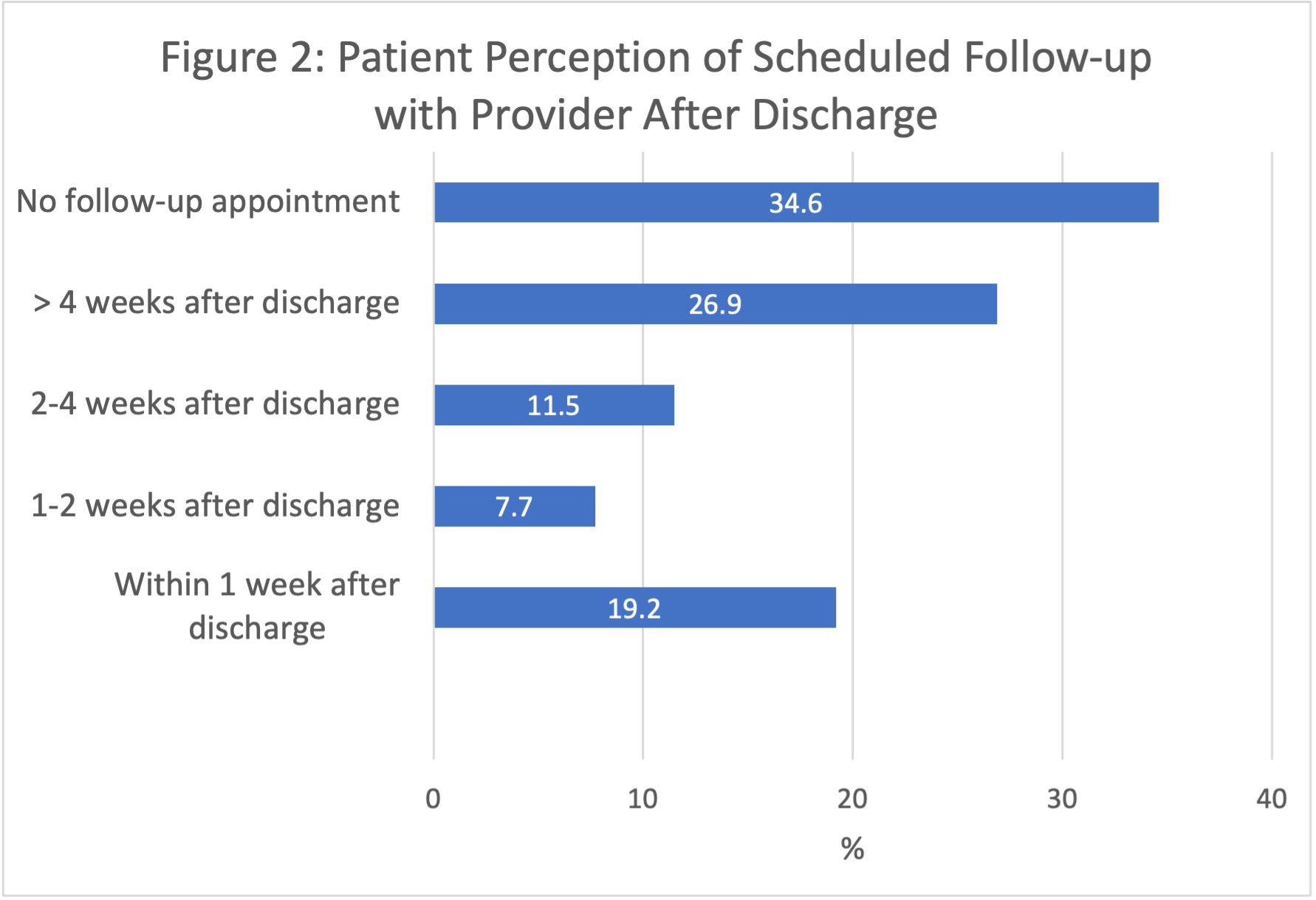
Results: A total of 72 patients with COVID-19 required new home oxygen. The 30-day readmission rate was 11.1% in this cohort, compared to 7.8% for all COVID-19 patients on the Medicine Service during the same period. 22% were scheduled for follow-up with a PCP only, 19% with a pulmonologist only, and 46% with both. 38% had a scheduled appointment within 7 days of discharge and 78% within 30 days. Only 23 (32%) received written instructions describing who to contact for concerns about equipment. 17 (24%) were referred to a remote oxygen monitoring program. Of the 72 patients, 26 (36%) agreed to participate in the phone survey. 58% expressed satisfaction with the discharge process (Fig. 1) and 24 (92%) reported feeling at least moderately prepared to use home oxygen. 5 (20%) patients expressed that the process was rushed and desired more education prior to discharge. 10 (38%) patients reported receiving no equipment education while hospitalized and receiving only in-home education by the equipment supplier. Equipment problems at the home were reported by 3 (8%) patients. Patients perceived wide variability in time to follow-up. 19% recalled follow-up within 1 week, 27% reported follow-up more than 4 weeks after discharge, and 35% reported lack of any follow-up appointment (Fig. 2). Chart review identified that most (19, 79%) had been scheduled for follow-up appointment within 30 days. 9 (35%) reported using the equipment less than 4 weeks, while 9 (35%) continued oxygen use beyond 3 months.
Conclusions: Our study found that patients hospitalized with COVID-19 requiring initiation of home oxygen had a higher 30-day readmission rate compared to all patients hospitalized with COVID-19, suggesting that this population is higher risk for adverse outcomes and requires careful discharge planning. Though most patients were satisfied with the process, approximately 20% felt the process was rushed and 40% did not receive education on the equipment while hospitalized. We also identified dissonance between patients’ perception of their follow-up and the follow-up appointments in the EHR. Based on the identification of these vulnerabilities in the transition process, our center plans to target additional processes for these patients, including enhanced early patient education, standard written discharge instructions, provision or prescription of pulse-oximeters, and standardization of post-discharge provider follow-up.