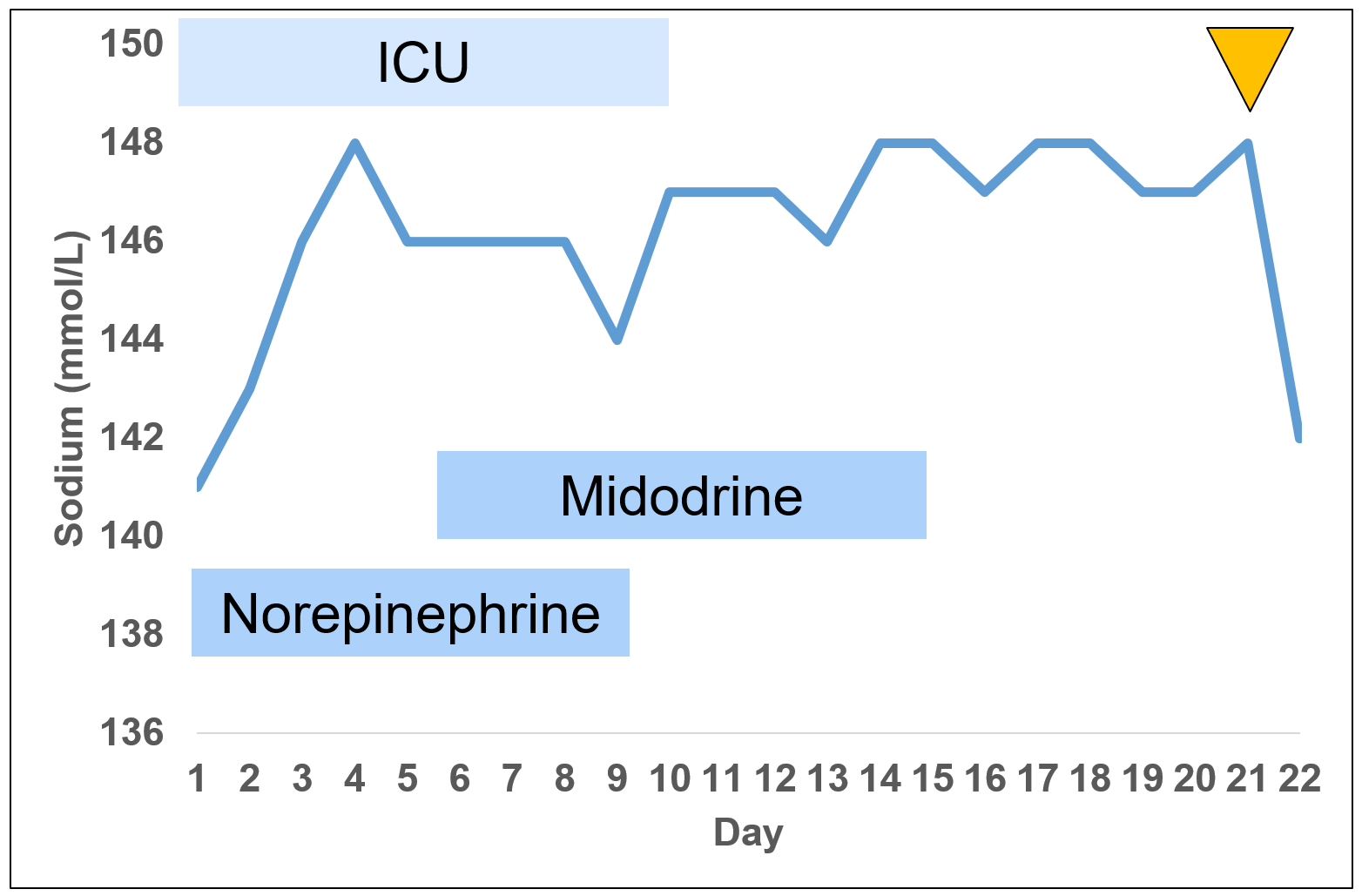
Case Presentation: A 73-year-old with history of Cushing’s disease status post left adrenalectomy presented to the emergency department with severe weakness, increased thirst and dizziness for one week. On presentation, her blood pressure was 89/67 and heart rate was 106. On exam, she appeared hypovolemic with dry mucous membranes. Initial laboratory studies showed a sodium of 137 mmol/L, bicarbonate 9 mmol/L, creatinine 0.6 mg/dL, glucose 215 mg/dL, lactate 2.9 mmol/L, and pH 7.39. She was given three liters of intravenous fluids with minimal urine output. She was transferred to the intensive care unit (ICU) for undifferentiated shock and started on norepinephrine and antibiotics. She remained intermittently hypotensive requiring norepinephrine for nine days. Her workup was negative for infection, adrenal insufficiency, and ventricular or valvular abnormalities. After 10 days in the ICU, she was transferred to intermediate care on high dose midodrine. She improved clinically though continued to have persistent hypernatremia, which had started on hospital day two. Serum sodium remained 147-148 mmol/L for two weeks despite aggressive fluid resuscitation and adequate oral intake of at least two liters of water per day despite minimal thirst. Serum osmolality was elevated at 303 and her urine osmolality was 137, consistent with water diuresis and raising concern for arginine vasopressin (AVP) deficiency. On further review of her outside records, she was found to have a history of non-functional pituitary macroadenoma diagnosed in 2018 by MRI; however, surveillance MRI imaging had not been feasible since the implantation of a spinal stimulator. Indirect water-deprivation test was performed, and her sodium normalized after administration of desmopressin, consistent with partial AVP deficiency. Unfortunately, repeat computed tomography head showed enlargement of the pituitary macroadenoma, likely the cause of her new AVP deficiency. She was weaned off midodrine and discharged home with desmopressin and follow up for neurosurgical resection.
Discussion: Hospitalized patients frequently develop hypernatremia related to increased water losses from third spacing, gastrointestinal losses, and diuresis as well as reduction of their free water intake. This case presentation of AVP deficiency was unusual as it presented with refractory hypotension for days in the ICU related to volume depletion, a lack of thirst despite hypernatremia, normal urine output, and inability to correct hypernatremia with dramatic increase in oral free water intake. While AVP deficiency and AVP resistance are generally characterized by polyuria and significant hypernatremia, partial AVP deficiency can present with more subtle clinical findings. The use of a water deprivation test was essential in establishing the diagnosis of partial AVP deficiency and normalizing the serum sodium. Although AVP deficiency and AVP resistance are generally characterized by polyuria and significant hypernatremia, partial AVP deficiency can present with more subtle findings such as mild hypernatremia that does not improve with fluids.
Conclusions: Though hospital-acquired hypernatremia is common, hospitalists should consider AVP deficiency and AVP resistance in cases of persistent hypernatremia and be familiar with the diagnostic tests including water deprivation testing and copeptin measurements. This case also highlights the pitfalls of anchoring bias and the value of obtaining outside records when encountering diagnostic dilemmas.