Background: Point-of-care ultrasound (POCUS) of the inferior vena cava (IVC) can help to noninvasively predict the effectiveness of treatment for volume-sensitive conditions, such as acute heart failure and shock. Recently POCUS-IVC has also been used to iteratively tailor fluid treatment to patient-specific targets. In real-world clinical settings, such iterative assessments are necessarily obtained by multiple different providers across multiple handoffs. Therefore, in order to be useful, the reliability of POCUS-IVC measurements obtained between observers must be high. We sought to determine the ‘best-case’ interobserver reliability of POCUS-IVC measurements and to determine whether expected clinical changes from fluid removal or infusion could be confidently distinguished from measurement error.
Methods: Our study occurred during the “POCUS for the Hospitalist” pre-course at the 2018 Society of Hospital Medicine national meeting. We enlisted 12 national POCUS experts to obtain measurements from 12 healthy subjects. Each subject remained supine on a gurney next to a POCUS machine equipped with a phased-array transducer. Blinded to others’ measurements, experts rotated in random order and were given 5 minutes to obtain and record measurements of the maximum and minimum IVC diameters from a long axis view while subjects breathed normally. We calculated within-subject standard deviations (Sws) for the 12 experts’ measurements of each diameter type and used multilevel modeling to pool these within-subject standard deviations across subjects. We then calculated ranges of repeatability as our measures of interobserver reliability. These ranges (calculated as 2 × √2 × 1.96 × Sws) are expected to contain 95% of the differences between two measurements on the same subject. Such ranges are clinically useful because only differences that lie outside of them can be confidently distinguished from measurement error. We used published estimates (Figure) to determine the average changes in IVC diameters with diuresis for acute heart failure (average weight loss of 3.6 kg over 8.5 days) and fluid resuscitation (0.9% normal saline bolus of 10 mL/kg over 30 minutes).
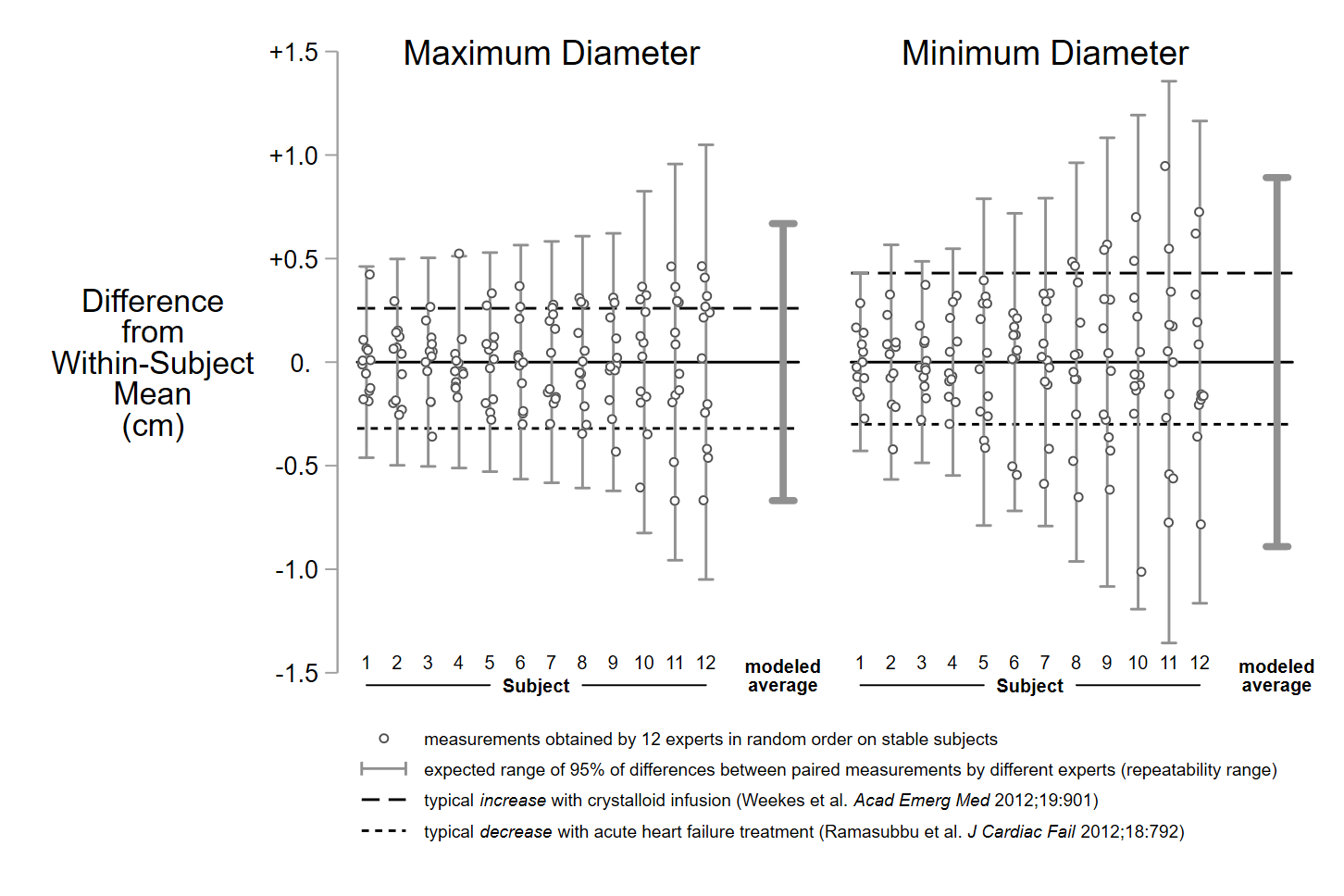
Results: As depicted in the Figure, every subject’s repeatability range for both their maximum and minimum IVC diameters exceeded the expected average decreases from diuresis and the expected average increases from crystalloid infusions. The upper and lower bounds of the average repeatability ranges for maximum and minimum diameters exceeded expected average changes from diuresis or resuscitation by approximately 0.5 cm.
Conclusions: Among national experts POCUS-IVC measurements have poor interobserver reliability. This calls into question the usefulness of quantitative POCUS-IVC measurements to track intravascular volume across providers.