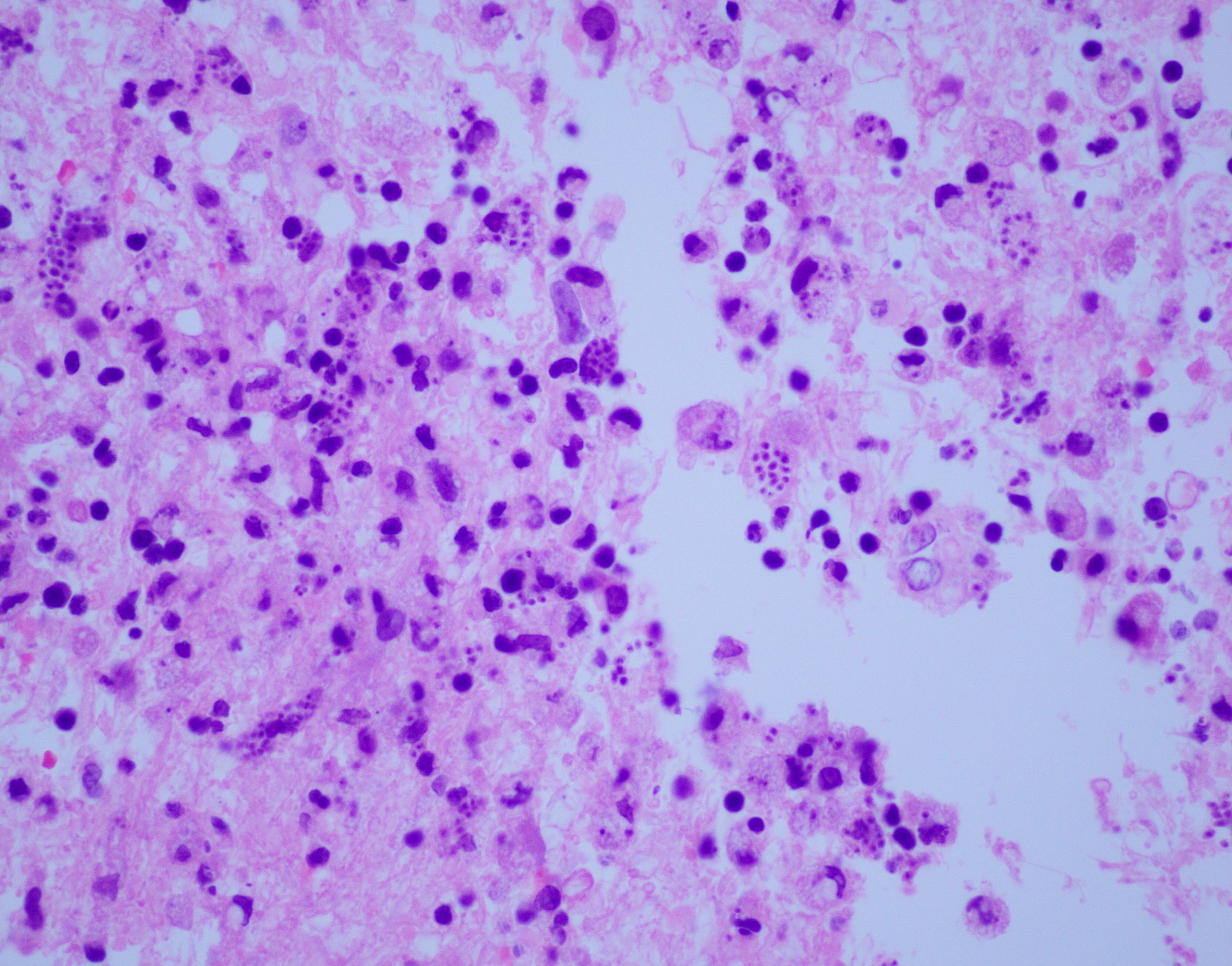
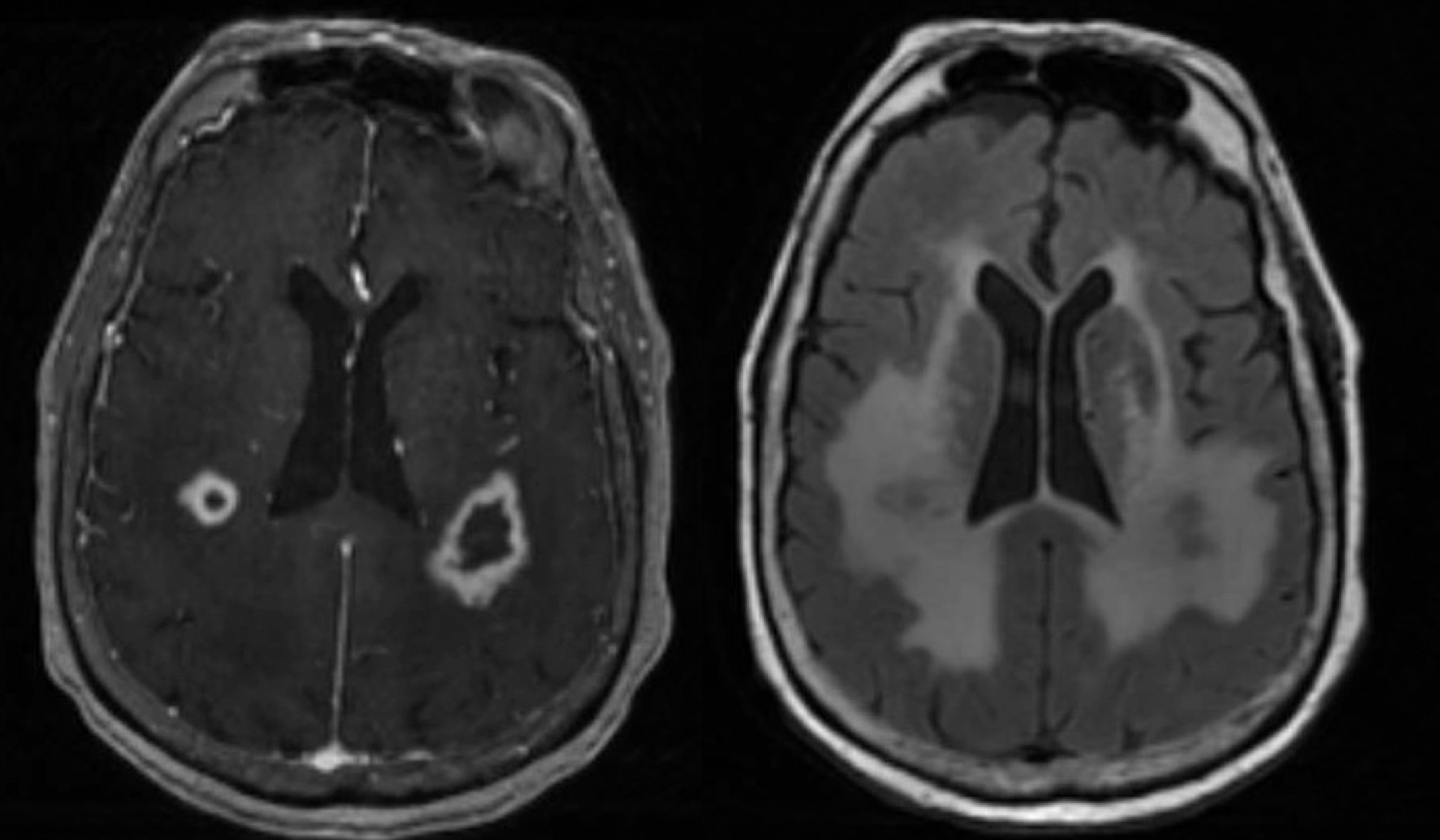
Case Presentation: An 88-year-old female from Peru with history of hypothyroidism, rheumatoid arthritis treated with oral methotrexate, and multiple recent transient ischemic attacks presented with altered mental status, difficulty speaking, and right sided weakness. The patient was unable to fully participate in any examination or conversation. Initial labs, including HIV tests, were unremarkable and head MRI demonstrated bilateral white matter lesions with thick, peripheral enhancing located within the frontoparietal regions causing extensive edematous changes. At this point, the differential included bacterial or fungal infections, primary CNS lymphoma, metastatic disease, multiple sclerosis, posterior reversible encephalopathy syndrome, or acute disseminated encephalomyelitis. A lumbar puncture found elevated lymphocytes, no oligoclonal bands, and negative bacterial and viral serology; brain biopsy demonstrated intracellular parasites which prompted PCR of the sample for Trypanosoma cruzi (T. cruzi.) After confirmation with the CDC, the patient received two weeks of benznidazole therapy before dying of respiratory failure.
Discussion: Diffuse, enhancing lesions on MRI with edematous changes requires a broad differential with a plan to differentiate between malignancy and infections. Specifically, primary CNS lymphoma and bacterial abscesses should be considered. In the absence of obvious infectious signs, brain biopsy may be required. Despite their infrequency, intracellular parasitic infections must be considered once other, more common, diagnoses are ruled out. Chagas disease is due to a secondary reactivation of T. cruzi and is most frequently seen in individuals from Latin America. While commonly causing cardiac and intestinal complications, T. cruzi has also been known to cause cerebral illness, most notably in immunosuppressed patients. Diagnosis of cerebral Chagas necessitates ruling out more common pathologies and a high clinical suspicion.
Conclusions: If T. cruzi is identified, it is necessary to begin directed anti-parasitic medications despite limited effectiveness against chronic disease. Perhaps due to this patient’s methotrexate history, Trypanosoma cruzi was able to indolently reactivate. This case exemplifies the necessity of a broad differential, a thorough history, and the diagnostic difficulties of imaging changes.