Background: Patients who complete a primary care provider (PCP) follow-up visit within 7 days of hospital discharge have lower odds of 14-day readmission (p=0.002) OR= 0.45 (95% CI: 0.27 – 0.73) compared to patients who do not at our academic institution. However, only 44% of patients complete this visit. Patients who were scheduled with their assigned PCP had higher odds of visit completion (P< 0.001) OR=1.68 (95% CI:1.37-2.06). Our aim was to better understand health system and patient facing barriers to timely scheduling of visits by building a structure to inform quality improvement efforts.
Methods: We implemented a multi-intervention quality improvement initiative in cross-departmental collaboration with operations, ambulatory care management, and scheduling teams. The initiative focused on 1) communicating with teams about the benefits of patients completing post-hospital discharge PCP follow-up visits with their assigned PCP; 2) streamlining the discharge-to-follow-up process through developing scheduling protocols to target scheduling patients with their assigned PCP within 7 days of hospital discharge; and 3) developing a Smart Form in the electronic health record for schedulers to capture real-time health system and patient-level scheduling barriers. We used Plan-Do-Study-Act (PDSA) cycles to refine the form to improve accuracy of barrier classification, usability, and reliability. Using longitudinal tracking of scheduling barrier data, the team identified areas for improvement and implemented further targeted interventions.
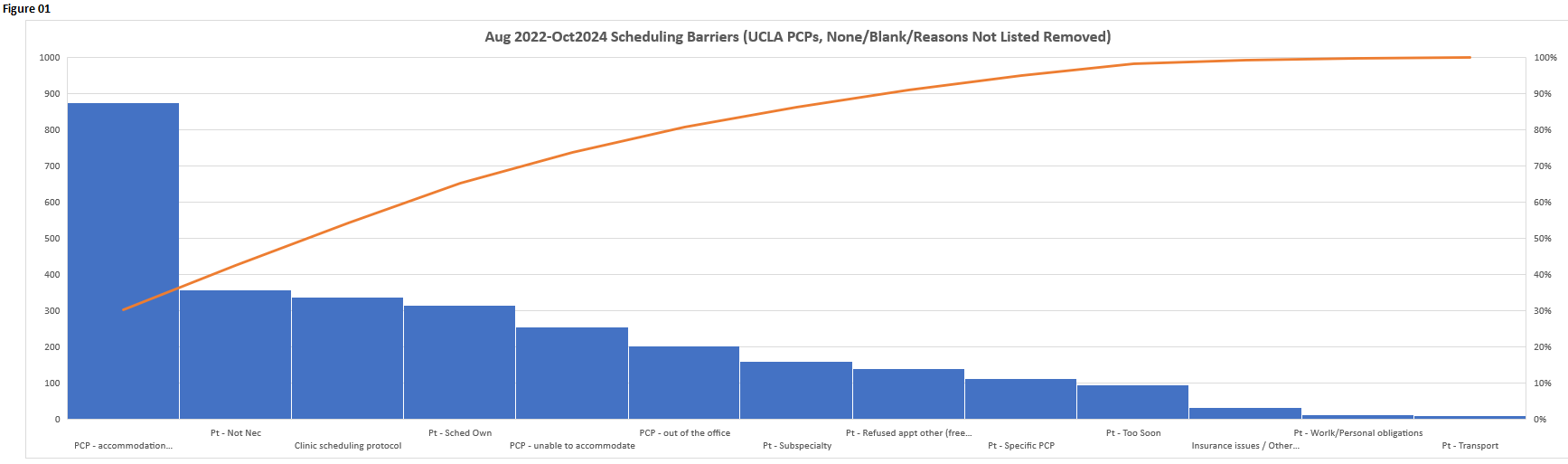
Results: From August 2022 through October 2024, schedulers used the Smart Form to document scheduling for 13,420 patients. 13,823 notes were made, of which 30% were documented with any type of barrier. Of 2,896 known/listed barriers, the most frequent barriers were PCP availability within target time frame (46%) and patient preferences (41%). Based on identification of PCP availability as a barrier, we introduced protected slots for post-hospital follow-up visits into PCP schedules. Informed by opportunities to support patients during this transition period, we 1) educated staff on utilizing protected slots to highlight the importance of the PCP follow-up visit; 2) piloted video encounters with the patient and scheduler prior to discharge to educate and encourage patient buy-in for scheduling and visit completion, 3) conducted a current state analysis identifying social determinants of health factors contributing to post-discharge scheduling and completion, and 4) facilitated outreach and education on Clinic Directors and their staff for accommodations and education on follow-up visits.
Conclusions: By leveraging interdisciplinary collaboration, real-time monitoring and documentation, and iterative PDSA cycles, we identified key scheduling barriers for post-discharge PCP visits that informed targeted interventions. Ongoing use of the Smart Form allows trending of overall and specific barriers to monitor the effectiveness of interventions. We harnessed existing scheduling workflows to introduce collaboration with schedulers in patient care improvement efforts. Using principles of data transparency, alignment of efforts, and continuous feedback, we formed a cross-department quality improvement team. Our findings underscore the importance of structured, data-driven quality improvement efforts in enhancing patient-centered care and continuity as well as including all members of the health care delivery team in improvement efforts.