Background: Skin, soft tissue, and joint infections are common in pediatric patients and can require invasive procedures to drain purulent fluid. Atypical pathogens (fungal and acid-fast bacilli [AFB]) are important but rare causes of these infections with reported case rates as low as 0.6-1.6 cases/100,000 a year. Despite the rarity of these infections, costly atypical cultures are often sent. Prior studies have shown the use of assessment tools decrease variability in care and aid in optimizing resource utilization. The objective of this study was to investigate the possibility of improving appropriate use of atypical cultures by (1) creating an Atypical Pathogen Assessment Protocol (APAP) and (2) validating its sensitivity in detecting atypical infections in pediatric patients over a 10 year period.
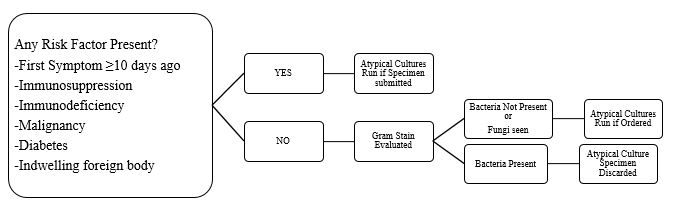
Methods: Utilizing recent literature and local experience with pediatric atypical infection epidemiology, 6 risk factors were identified for a risk assessment tool: symptoms for 10 days or more, immunosuppression, immunodeficiency, malignancy, diabetes, or indwelling foreign body. This tool combined with gram stain results constituted a 2-tiered screening protocol (APAP: Figure). To test the sensitivity of APAP, we conducted a retrospective chart review of all patients at a single freestanding children’s hospital with positive atypical cultures over 10 years (2009-2018). APAP was retrospectively applied to patients with cultures from potentially infected fluid in normally sterile sites, such as bone, joint, or soft tissue aspirates. Patients were excluded if cultures were obtained from normally non-sterile sites (respiratory tract, GI tract lumen, skin swabs) or from solid tissue specimens.
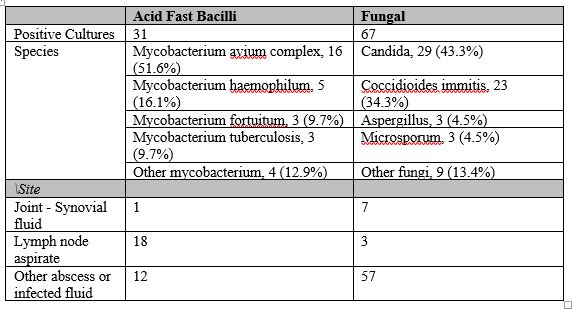
Results: 19,632 cultures were obtained and 1732 (8.8%) resulted positive for fungal or AFB species; 98 cultures met inclusion criteria (Table). Patient ages ranged from 12 days to 18 years (mean 8.6 years) and 52% were male. The 2-tiered risk assessment protocol was 100% sensitive in identifying patients with positive atypical cultures. All patients with tuberculosis, non-tubercular mycobacteria, Coccidioidomycosis, and non-Candida fungal infections were identified by the risk factors alone. Gram stain identified 4 additional cases positive for Candida, all of which had positive bacterial cultures and were treated with antibiotics; 1 patient was treated with antifungals. Three of the 4 cases grew only a single colony of Candida making the clinical significance of the gram stain findings questionable.
Conclusions: APAP was 100% sensitive in identifying patients with positive atypical cultures in our study population over a 10 year period, and therefore offers promise in 2 areas: 1) To guide the proceduralist in the decision whether to order atypical cultures when draining potentially infected fluid, and 2) To decrease processing of low-yield fluid specimens in the microbiology lab when bacteria are seen on gram stains in patients without risk factors for atypical infections. Additional matched case control analysis is planned to evaluate specificity of APAP.